Academic Neurology, Nottingham University Hospitals NHS Trust, Nottingham, United Kingdom; Mental Health and Clinical Neurosciences Academic Unit, School of Medicine, University of Nottingham, Nottingham, United Kingdom.
Direct Commissioning, National Health Services Arden and Greater East Midlands Commissioning Support Unit, Leicester, United Kingdom.
Mult Scler Relat Disord. 2022 Jan;57:103458. doi: 10.1016/j.msard.2021.103458. Epub 2021 Dec 5.
Contradicting assumptions have been made about the effectiveness of SARS-CoV-2 vaccines in patients with multiple sclerosis (MS) receiving immunomodulatory disease-modifying therapies (DMTs) based on the quantification of humoral and cellular immune responses. This study aimed to understand changes in the risk of SARS-CoV-2 infection among the total population of patients receiving MS DMTs in England following mass vaccination.
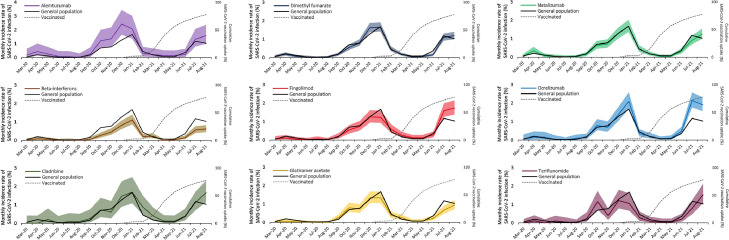
This is a retrospective analysis of national data collected prospectively and longitudinally. National Health Service (NHS) England and NHS Improvement (NHSE/I) hold prescribing data on all commissioned MS DMTs in England. United Kingdom Health Security Agency (UKHSA) has been collecting data on all registered SARS-CoV-2 test results, including polymerase chain reaction and rapid antigen tests. All patients receiving MS DMTs were identified using NHSE/I datasets. All patients receiving MS DMTs with SARS-CoV-2 infection (i.e., positive test) from March 2020 to August 2021 were identified by merging NHSE/I and UKHSA datasets. Similar data for the general population were captured using publicly available datasets of the United Kingdom government. The incidence rate ratios (IRR) of SARS-CoV-2 infection among patients receiving MS DMTs compared to the general population during the pre-vaccination (November 2020 to January 2021) and post-vaccination (June to August 2021) periods were calculated.
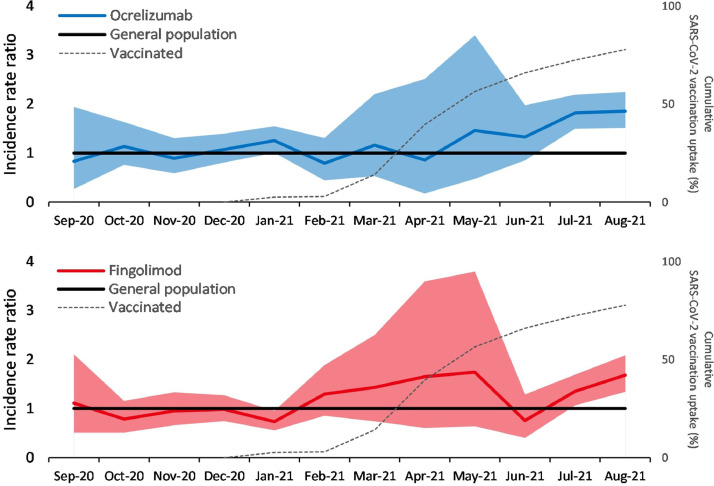
A mean (standard deviation) of 41,208 (4,301) patients received an MS DMT in England during each month from March 2020 to August 2021. The IRR (95% confidence interval) of infection in patients taking ocrelizumab versus the general population increased from 1.13 (0.97-1.31) during the pre-vaccination period to 1.79 (1.57-2.03) during the post-vaccination period. For patients on fingolimod, it increased from 0.87 (0.73-1.02) to 1.40 (1.20-1.63) during the same periods. There were no significant changes for patients on other MS DMTs.
SARS-CoV-2 vaccines offer less protection against infection to patients taking ocrelizumab or fingolimod, who have an impaired immune response to vaccines, than the general population. These findings will have implications for vaccination policies.
根据体液和细胞免疫反应的定量分析,人们对接受免疫调节疾病修正治疗 (DMT) 的多发性硬化症 (MS) 患者中 SARS-CoV-2 疫苗的有效性做出了相互矛盾的假设。本研究旨在了解在英格兰大规模接种疫苗后,接受 MS DMT 的患者总数中 SARS-CoV-2 感染风险的变化。
这是一项对前瞻性和纵向收集的全国数据进行的回顾性分析。英格兰国民保健署 (NHS) 和 NHS 改进 (NHSE/I) 保存了所有在英格兰开处方的 MS DMT 的用药数据。英国卫生安全局 (UKHSA) 一直在收集所有注册的 SARS-CoV-2 检测结果的数据,包括聚合酶链反应和快速抗原检测。使用 NHSE/I 数据集确定接受 MS DMT 的所有患者。通过合并 NHSE/I 和 UKHSA 数据集,确定 2020 年 3 月至 2021 年 8 月期间接受 MS DMT 且发生 SARS-CoV-2 感染(即检测呈阳性)的所有患者。使用英国政府提供的公开数据集获取接受 MS DMT 的患者的一般人群的相似数据。计算接种疫苗前(2020 年 11 月至 2021 年 1 月)和接种疫苗后(2021 年 6 月至 8 月)期间与普通人群相比,接受 MS DMT 的患者 SARS-CoV-2 感染的发病率比值 (IRR)。
2020 年 3 月至 2021 年 8 月期间,英格兰平均每月有 41208(4301)名患者接受 MS DMT。与普通人群相比,接受奥瑞珠单抗治疗的患者感染的 IRR(95%置信区间)从接种疫苗前的 1.13(0.97-1.31)增加到接种疫苗后的 1.79(1.57-2.03)。对于接受 fingolimod 的患者,该比值从 0.87(0.73-1.02)增加到 1.40(1.20-1.63)。其他 MS DMT 患者的比值没有明显变化。
SARS-CoV-2 疫苗对免疫反应受损的接受 ocrelizumab 或 fingolimod 治疗的患者的感染提供的保护作用低于普通人群。这些发现将对疫苗接种政策产生影响。