Heinzmann Alexandra C A, Coenen Daniëlle M, Vajen Tanja, Cosemans Judith M E M, Koenen Rory R
Department of Biochemistry, Cardiovascular Research Institute Maastricht (CARIM), Maastricht University, Maastricht, the Netherlands.
Department of Molecular and Cellular Biochemistry, University of Kentucky College of Medicine, Lexington, Kentucky, United States.
TH Open. 2021 Oct 28;5(4):e533-e542. doi: 10.1055/a-1682-3415. eCollection 2021 Oct.
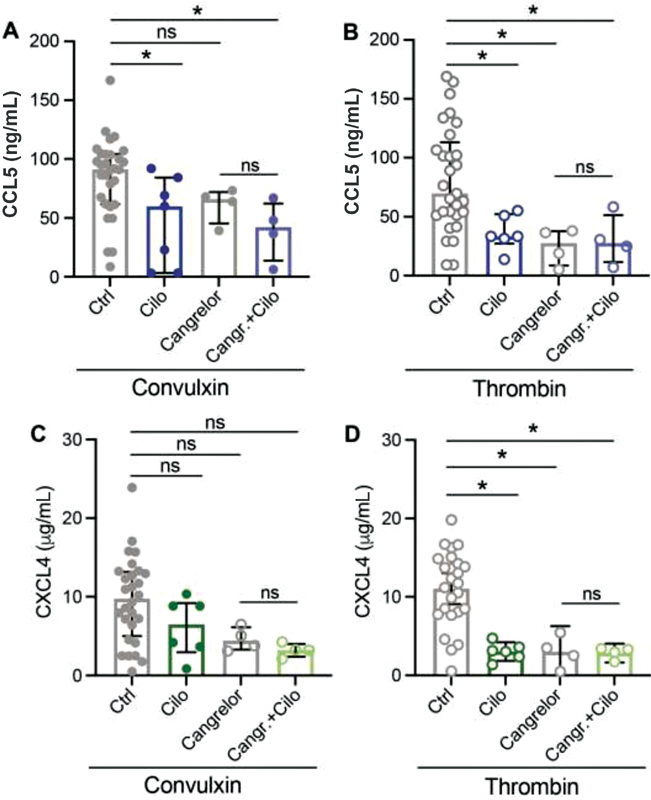
The cause of atherothrombosis is rupture or erosion of atherosclerotic lesions, leading to an increased risk of myocardial infarction or stroke. Here, platelet activation plays a major role, leading to the release of bioactive molecules, for example, chemokines and coagulation factors, and to platelet clot formation. Several antiplatelet therapies have been developed for secondary prevention of cardiovascular events, in which anticoagulant drugs are often combined. Besides playing a role in hemostasis, platelets are also involved in inflammation. However, it is unclear whether current antiplatelet therapies also affect platelet immune functions. In this study, the possible anti-inflammatory effects of antiplatelet medications on chemokine release were investigated using enzyme-linked immunosorbent assay and on the chemotaxis of THP-1 cells toward platelet releasates. We found that antiplatelet medication acetylsalicylic acid (ASA) led to reduced chemokine (CC motif) ligand 5 (CCL5) and chemokine (CXC motif) ligand 4 (CXCL4) release from platelets, while leukocyte chemotaxis was not affected. Depending on the agonist, α β and P2Y inhibitors also affected CCL5 or CXCL4 release. The combination of ASA with a P2Y inhibitor or a phosphodiesterase (PDE) inhibitor did not lead to an additive reduction in CCL5 or CXCL4 release. Interestingly, these combinations did reduce leukocyte chemotaxis. This study provides evidence that combined therapy of ASA and a P2Y or PDE3 inhibitor can decrease the inflammatory leukocyte recruiting potential of the releasate of activated platelets.
动脉粥样硬化血栓形成的原因是动脉粥样硬化病变的破裂或糜烂,导致心肌梗死或中风的风险增加。在此过程中,血小板活化起主要作用,导致生物活性分子如趋化因子和凝血因子的释放,并形成血小板凝块。已经开发了几种抗血小板疗法用于心血管事件的二级预防,其中抗凝药物常联合使用。除了在止血中发挥作用外,血小板还参与炎症反应。然而,目前的抗血小板疗法是否也会影响血小板的免疫功能尚不清楚。在本研究中,使用酶联免疫吸附测定法研究了抗血小板药物对趋化因子释放的可能抗炎作用,以及THP-1细胞对血小板释放物的趋化作用。我们发现抗血小板药物乙酰水杨酸(ASA)可减少血小板趋化因子(CC基序)配体5(CCL5)和趋化因子(CXC基序)配体4(CXCL4)的释放,而白细胞趋化性未受影响。根据激动剂的不同,αβ和P2Y抑制剂也会影响CCL5或CXCL4的释放。ASA与P2Y抑制剂或磷酸二酯酶(PDE)抑制剂联合使用不会导致CCL5或CXCL4释放的额外减少。有趣的是,这些联合用药确实降低了白细胞趋化性。本研究提供了证据,表明ASA与P2Y或PDE3抑制剂联合治疗可降低活化血小板释放物的炎性白细胞募集潜能。