Bisquera Alessandra, Turner Ellie Bragan, Ledwaba-Chapman Lesedi, Dunbar-Rees Rupert, Hafezparast Nasrin, Gulliford Martin, Durbaba Stevo, Soley-Bori Marina, Fox-Rushby Julia, Dodhia Hiten, Ashworth Mark, Wang Yanzhong
King's College London, School of Population Health & Environmental Sciences, London, UK.
NIHR Biomedical Research Centre, Guy's and St Thomas' NHS Foundation Trust and King's College London, London, UK.
Lancet Reg Health Eur. 2021 Nov 4;12:100247. doi: 10.1016/j.lanepe.2021.100247. eCollection 2022 Jan.
Social and material deprivation accelerate the development of multimorbidity, yet the mechanisms which drive multimorbidity pathways and trajectories remain unclear. We aimed to examine the association between health inequality, risk factors and accumulation or resolution of LTCs, taking disease sequences into consideration.
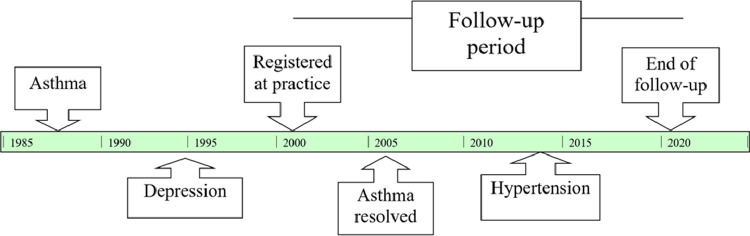
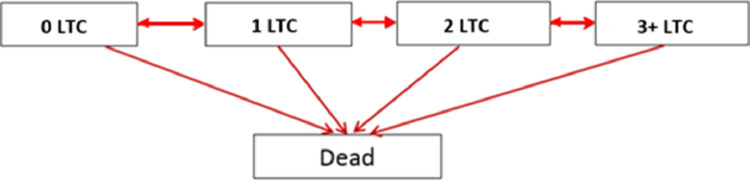
We conducted a retrospective cohort of adults aged 18 years and over, registered between April 2005 and May 2020 in general practices in one inner London borough ( = 826,936). Thirty-two long term conditions (LTCs) were selected using a consensus process, based on a definition adapted to the demographic characteristics of the local population. sThe development and resolution of these LTCs were examined according to sociodemographic and clinical risk factors (hypertension; moderate obesity (BMI 30·0-39·9 kg/m2), high cholesterol (total cholesterol > 5 mmol/L), smoking, high alcohol consumption (>14 units per week), and psychoactive substance use), through the application of multistate Markov chain models.
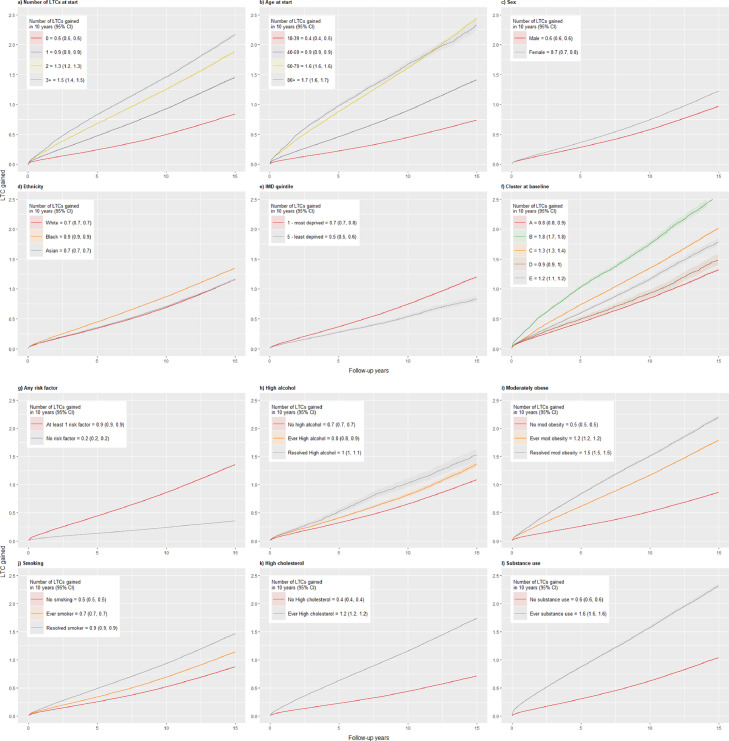
Participants were followed up for a median of 4.2 years (IQR = 1·8 - 8·4); 631,760 (76%) entered the study with no LTCs, 121,424 (15%) with 1 LTC, 41,720 (5%) with 2 LTCs, and 31,966 (4%) with three or more LTCs. At the end of follow-up, 194,777 (24%) gained one or more LTCs, while 45,017 (5%) had resolved LTCs and 27,021 (3%) died. In multistate models, deprivation (hazard ratio [HR] between 1·30 to 1·64), female sex (HR 1·13 to 1·20), and Black ethnicity (HR 1·20 to 1·30; vs White) were independently associated with increased risk of transition from one to two LTCs, and shorter time spent in a healthy state. Substance use was the strongest risk factor for multimorbidity with an 85% probability of gaining LTCs over the next year. First order Markov chains identified consistent disease sequences including: chronic pain or osteoarthritis followed by anxiety and depression; alcohol and substance dependency followed by HIV, viral hepatitis, and liver disease; and morbid obesity followed by diabetes, hypertension, and chronic pain.
We examined the relations among 32 LTCs, taking the order of disease occurrence into consideration. Distinctive patterns for the development and accumulation of multimorbidity have emerged, with increased risk of transitioning from no conditions to multimorbidity and mortality related to ethnicity, deprivation and gender. Musculoskeletal disorders, morbid obesity and substance abuse represent common entry points to multimorbidity trajectories.
社会和物质匮乏会加速多种疾病的发展,然而驱动多种疾病发生途径和发展轨迹的机制仍不清楚。我们旨在研究健康不平等、风险因素与长期病症(LTCs)的累积或缓解之间的关联,并考虑疾病顺序。
我们对2005年4月至2020年5月期间在伦敦市中心一个行政区的全科医疗中登记的18岁及以上成年人进行了一项回顾性队列研究(n = 826,936)。基于适应当地人口统计学特征的定义,通过共识过程选择了32种长期病症。根据社会人口统计学和临床风险因素(高血压;中度肥胖(BMI 30.0 - 39.9 kg/m²)、高胆固醇(总胆固醇>5 mmol/L)、吸烟、高酒精摄入量(每周>14单位)和精神活性物质使用),应用多状态马尔可夫链模型来研究这些长期病症的发生和缓解情况。
参与者的中位随访时间为4.2年(IQR = 1.8 - 8.4);631,760人(76%)进入研究时无长期病症,121,424人(15%)有1种长期病症,41,720人(5%)有2种长期病症,31,966人(4%)有三种或更多长期病症。在随访结束时,194,777人(24%)患上了一种或多种长期病症,而45,017人(5%)的长期病症得到缓解,27,021人(3%)死亡。在多状态模型中,匮乏(风险比[HR]在1.30至1.64之间)、女性(HR 1.13至1.20)和黑人种族(HR 1.20至1.30;与白人相比)与从一种长期病症转变为两种长期病症的风险增加以及在健康状态下花费的时间缩短独立相关。物质使用是多种疾病发生的最强风险因素,在接下来的一年中患上长期病症的概率为85%。一阶马尔可夫链确定了一致的疾病顺序,包括:慢性疼痛或骨关节炎后接着是焦虑和抑郁;酒精和物质依赖后接着是艾滋病毒、病毒性肝炎和肝病;病态肥胖后接着是糖尿病、高血压和慢性疼痛(疼痛)。
我们考虑了疾病发生顺序,研究了32种长期病症之间的关系。已经出现了多种疾病发生和累积的独特模式,从无病症转变为多种疾病以及与种族、匮乏和性别相关的死亡率风险增加。肌肉骨骼疾病、病态肥胖和药物滥用是多种疾病发展轨迹的常见切入点。