Research Department of Primary Care and Population Health, University College London (UCL), Rowland Hill Street, London, NW3 2PF, UK.
Escuela de Medicina, Universidad Cesar Vallejo, Trujillo, Peru.
Sci Rep. 2021 Dec 13;11(1):23826. doi: 10.1038/s41598-021-02670-9.
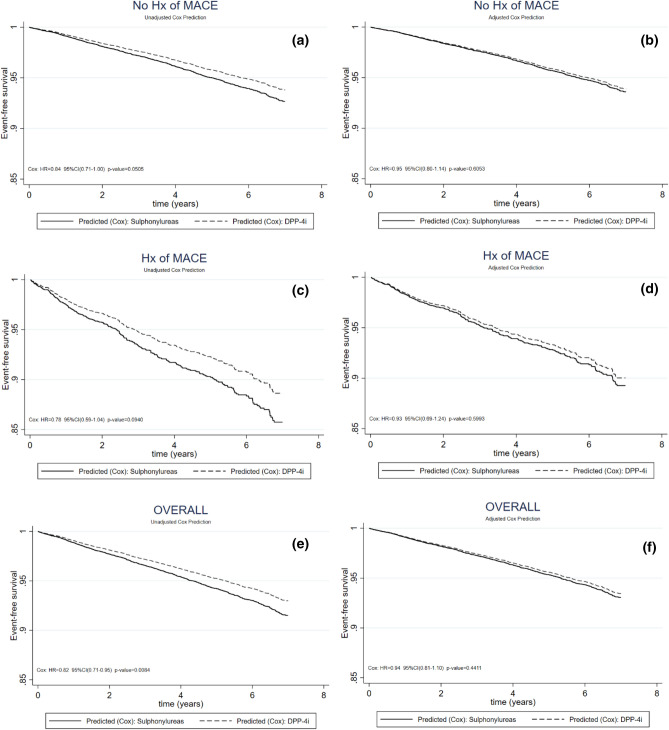
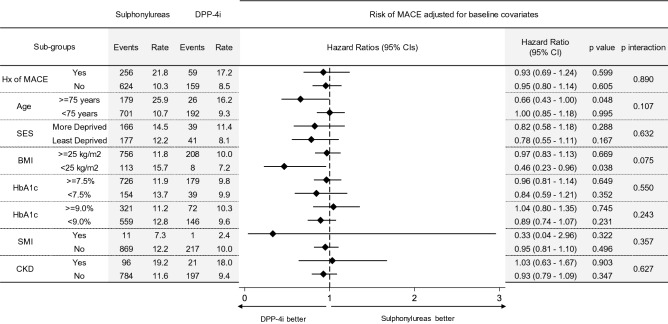
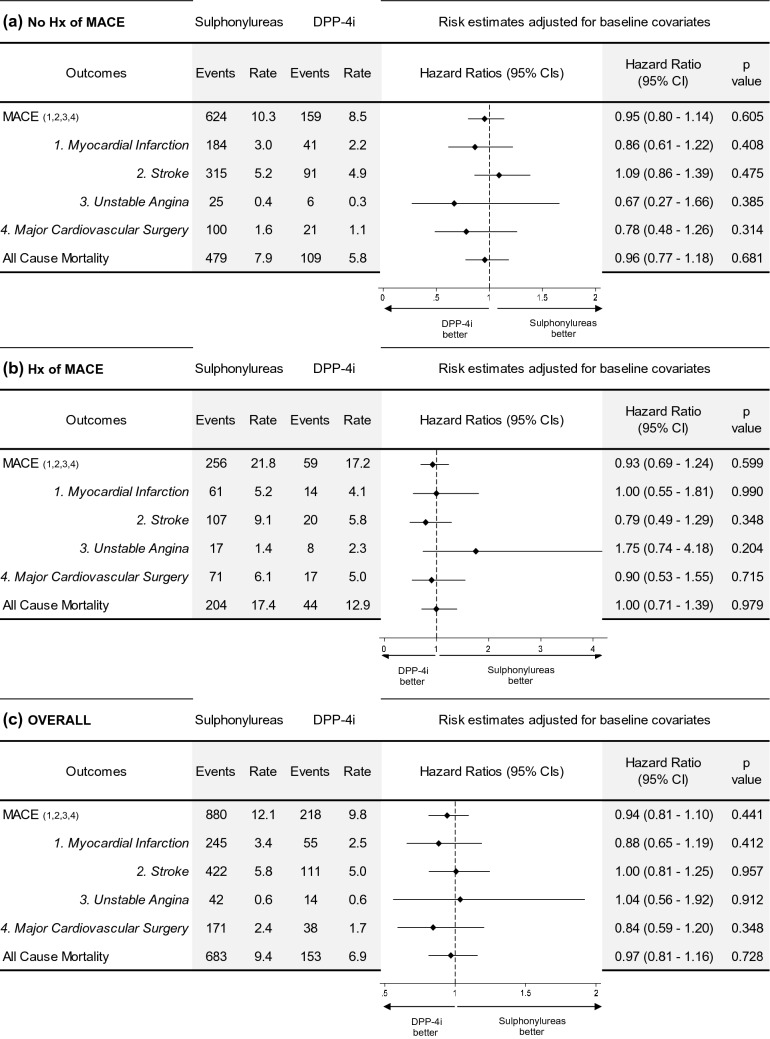
DPP-4 inhibitors (DPP-4i) and sulphonylureas remain the most widely prescribed add-on treatments after metformin. However, there is limited evidence from clinical practice comparing major adverse cardiovascular events (MACE) in patients prescribed these treatments, particularly among those without prior history of MACE and from vulnerable population groups. Using electronic health records from UK primary care, we undertook a retrospective cohort study with people diagnosed type-2 diabetes mellitus, comparing incidence of MACE (myocardial infarction, stroke, major cardiovascular surgery, unstable angina) and all-cause mortality among those prescribed DPP-4i versus sulphonylureas as add-on to metformin. We stratified analysis by history of MACE, age, social deprivation and comorbidities and adjusted for HbA1c, weight, smoking-status, comorbidities and medications. We identified 17,570 patients prescribed sulphonylureas and 6,267 prescribed DPP-4i between 2008-2017. Of these, 16.3% had pre-existing MACE. Primary incidence of MACE was similar in patients prescribed DPP-4i and sulphonylureas (10.3 vs 8.5 events per 1000 person-years; adjusted Hazard Ratio (adjHR): 0.94; 95%CI 0.80-1.14). For those with pre-existing MACE, rates for recurrence were higher overall, but similar between the two groups (21.8 vs 17.2 events per 1000 person-years; adjHR: 0.93; 95%CI 0.69-1.24). For those aged over 75 and with BMI less than 25 kg/m there was a protective effect for DPP-I, warranting further investigation. Patients initiating a DPP-4i had similar risk of cardiovascular outcomes to those initiating a sulphonylurea. This indicates the choice should be based on safety and cost, not cardiovascular prognosis, when deciding between a DPP-4i or sulphonylurea as add-on to metformin.
二肽基肽酶-4 抑制剂(DPP-4i)和磺脲类药物仍然是二甲双胍治疗后最广泛应用的附加治疗药物。然而,临床实践中比较使用这些药物的患者主要不良心血管事件(MACE)的证据有限,特别是在没有既往 MACE 史和脆弱人群中。本研究使用英国初级保健的电子健康记录,开展了一项回顾性队列研究,比较了诊断为 2 型糖尿病的患者中,使用 DPP-4i 与磺脲类药物作为二甲双胍附加治疗的 MACE(心肌梗死、中风、主要心血管手术、不稳定型心绞痛)发生率和全因死亡率。我们按 MACE 史、年龄、社会剥夺和合并症进行分层分析,并根据 HbA1c、体重、吸烟状况、合并症和药物进行调整。我们确定了 2008-2017 年间使用磺脲类药物和 DPP-4i 的患者各 17570 人和 6267 人。其中,16.3%的患者存在既往 MACE。使用 DPP-4i 和磺脲类药物的患者 MACE 的初级发生率相似(10.3 与 8.5 事件/1000 人年;调整后的危险比(adjHR):0.94;95%CI 0.80-1.14)。对于既往有 MACE 的患者,复发率总体较高,但两组之间相似(21.8 与 17.2 事件/1000 人年;adjHR:0.93;95%CI 0.69-1.24)。对于年龄超过 75 岁和 BMI 低于 25kg/m 的患者,DPP-1 有保护作用,需要进一步研究。起始使用 DPP-4i 的患者发生心血管结局的风险与起始使用磺脲类药物的患者相似。这表明在决定将 DPP-4i 或磺脲类药物作为二甲双胍的附加治疗时,应根据安全性和成本而不是心血管预后来选择。