Department of Epidemiology, Noguchi Memorial Institute for Medical Research, University of Ghana, Legon, Accra, Ghana.
Centre for Tropical Clinical Pharmacology and Therapeutics, University of Ghana Medical School, Accra, Ghana.
BMC Infect Dis. 2021 Dec 15;21(1):1255. doi: 10.1186/s12879-021-06961-4.
Since the introduction of artemisinin-based combination therapy (ACT) in Ghana in 2005 there has been a surveillance system by the National Malaria Control Programme (NMCP) and the University of Ghana Noguchi Memorial Institute for Medical Research (UG-NMIMR) to monitor the therapeutic efficacy of ACTs for the treatment of uncomplicated malaria in the country. We report trends and determinants of failure following treatment of Ghanaian children with artesunate-amodiaquine (ASAQ) and artemether-lumefantrine (AL) combinations.
Per protocol analyses as well as cumulative incidence of day 28 treatment failure from Kaplan Meier survival analyses were used to describe trends of failure over the surveillance period of 2005-2018. Univariable and multivariable cox regression analyses were used to assess the determinants of treatment failure over the period.
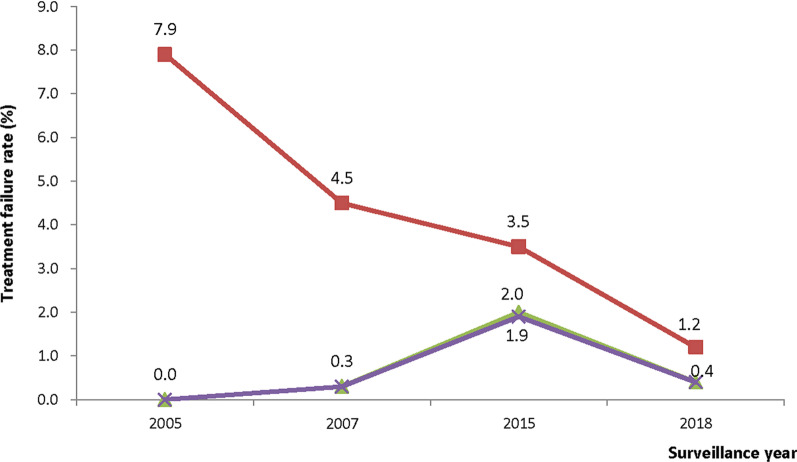
Day 28 PCR-corrected failure, following treatment with ASAQ, significantly increased from 0.0% in 2005 to 2.0% (95% CI: 1.1-3.6) in 2015 (p = 0.013) but significantly decreased to 0.4% (95% CI: 0.1-1.6) in 2018 (p = 0.039). Failure, following treatment with AL, decreased from 4.5% (95% CI: 2.0-9.4) in 2010 to 2.7% (95% CI: 1.4-5.1) in 2018, though not statistically significant (p = 0.426). Risk of treatment failure, from multivariable cox regression analyses, was significantly lower among children receiving ASAQ compared with those receiving AL (HR = 0.24; 95% CI: 0.11-0.53; p < 0.001); lower among children with no parasitaemia on day 3 compared with those with parasitaemia on day 3 (HR = 0.02; 95% CI: 0.01-0.13; p < 0.001); and higher among children who received ASAQ and had axillary temperature ≥ 37.5 °C on day 1 compared with those with axillary temperature < 37.5 °C (HR = 3.96; 95% CI: 1.61-9.75; p = 0.003).
Treatment failures for both ASAQ and AL have remained less than 5% (below WHO's threshold of 10%) in Ghana since 2005. Predictors of treatment failure that need to be considered in the management of uncomplicated malaria in the country should include type of ACT, day 3 parasitaemia, and day 1 axillary temperature of patients being treated.
自 2005 年加纳引入青蒿素为基础的联合疗法(ACT)以来,国家疟疾控制规划(NMCP)和加纳大学戈努希纪念医学研究所(UG-NMIMR)一直在通过监测系统监测 ACT 治疗该国无并发症疟疾的治疗效果。我们报告了使用青蒿琥酯-阿莫地喹(ASAQ)和青蒿素-本芴醇(AL)联合治疗加纳儿童后治疗失败的趋势和决定因素。
根据方案分析以及从 Kaplan-Meier 生存分析得出的第 28 天治疗失败的累积发生率,描述了 2005 年至 2018 年监测期间失败的趋势。使用单变量和多变量 Cox 回归分析评估了该期间治疗失败的决定因素。
第 28 天 PCR 校正失败率,使用 ASAQ 治疗后,从 2005 年的 0.0%显著增加到 2015 年的 2.0%(95%CI:1.1-3.6)(p=0.013),但在 2018 年显著下降至 0.4%(95%CI:0.1-1.6)(p=0.039)。使用 AL 治疗后的失败率从 2010 年的 4.5%(95%CI:2.0-9.4)下降到 2018 年的 2.7%(95%CI:1.4-5.1),尽管无统计学意义(p=0.426)。多变量 Cox 回归分析显示,与接受 AL 治疗的儿童相比,接受 ASAQ 治疗的儿童治疗失败的风险显著降低(HR=0.24;95%CI:0.11-0.53;p<0.001);第 3 天无寄生虫血症的儿童与第 3 天有寄生虫血症的儿童相比(HR=0.02;95%CI:0.01-0.13;p<0.001);与腋温<37.5°C的儿童相比,接受 ASAQ 治疗且腋温≥37.5°C的儿童(HR=3.96;95%CI:1.61-9.75;p=0.003)。
自 2005 年以来,加纳使用 ASAQ 和 AL 的治疗失败率一直低于 5%(低于世卫组织 10%的阈值)。在该国管理无并发症疟疾时需要考虑的治疗失败的预测因素应该包括 ACT 类型、第 3 天寄生虫血症和接受治疗的患者第 1 天的腋温。