Department of Community Health Sciences, Faculty of Medicine and Health Sciences, Université de Sherbrooke, 150, Place Charles-Le Moyne, C. P. 200, Longueuil, QC, J4K 0A8, Canada.
Centre de recherche Charles-LeMoyne, Université de Sherbrooke - Campus Longueuil, 150, place Charles-Le Moyne, C. P. 200, Longueuil, QC, J4K 0A8, Canada.
BMC Health Serv Res. 2021 Dec 16;21(1):1345. doi: 10.1186/s12913-021-07286-3.
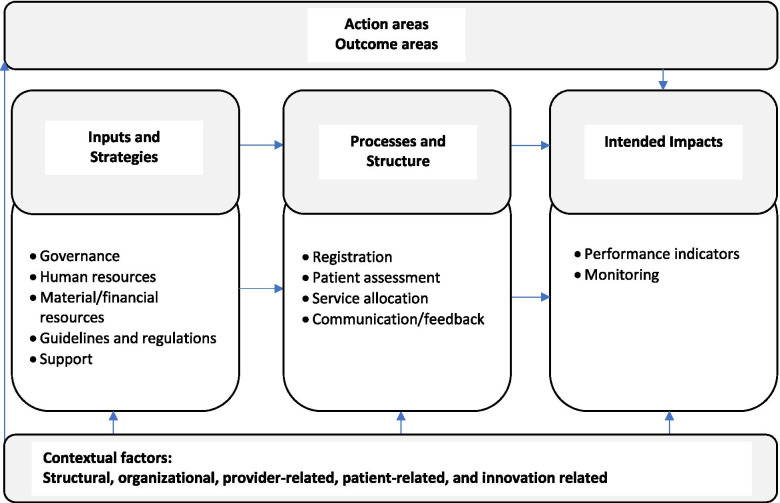
In 2016, Quebec, a Canadian province, implemented a program to improve access to specialized health services (Accès priorisé aux services spécialisés (APSS)), which includes single regional access points for processing requests to such services via primary care (Centre de répartition des demandes de services (CRDS)). Family physicians fill out and submit requests for initial consultations with specialists using a standardized form with predefined prioritization levels according to listed reasons for consultations, which is then sent to the centralized referral system (the CRDS) where consultations with specialists are assigned. We 1) described the APSS-CRDS program in three Quebec regions using logic models; 2) compared similarities and differences in the components and processes of the APSS-CRDS models; and 3) explored contextual factors influencing the models' similarities and differences.
We relied on a qualitative study to develop logic models of the implemented APSS-CRDS program in three regions. Semi-structured interviews with health administrators (n = 9) were conducted. The interviews were analysed using a framework analysis approach according to the APSS-CRDS's components included in the initially designed program, Mitchell and Lewis (2003)'s logic model framework, and Chaudoir and colleagues (2013)'s framework on contextual factors' influence on an innovation's implementation.
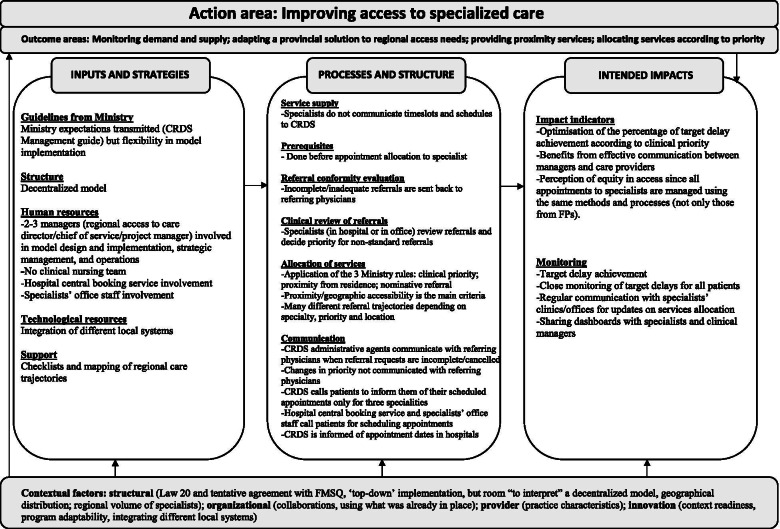
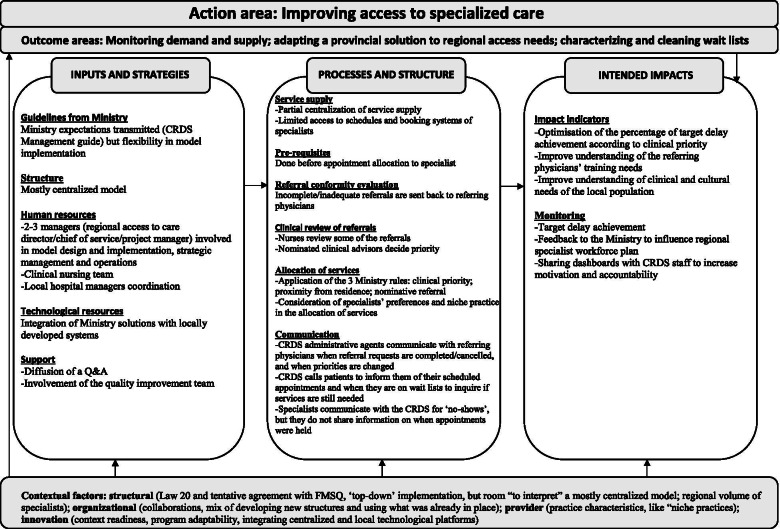
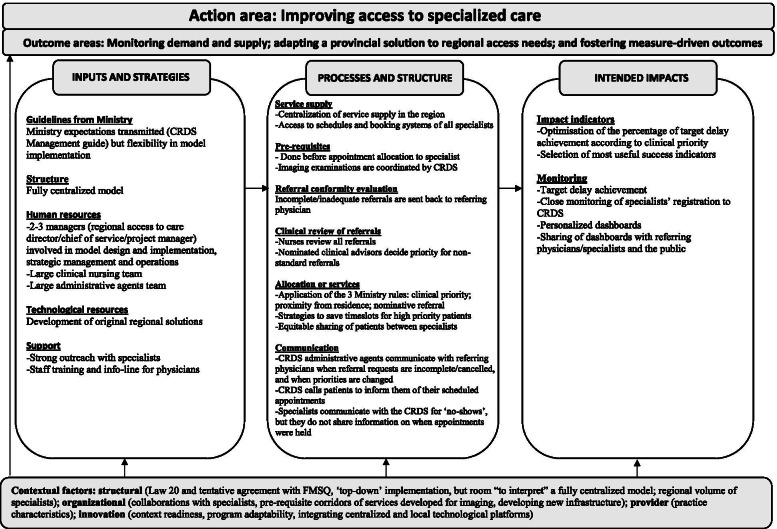
Findings show the APSS-CRDS program's regional variability in the implementation of its components, including its structure (centralized/decentralized), human resources involved in implementation and operation, processes to obtain specialists' availability and assess/relay requests, as well as monitoring methods. Variability may be explained by contextual factors' influence, like ministerial and medical associations' involvement, collaborations, the context's implementation readiness, physician practice characteristics, and the program's adaptability.
Findings are useful to inform decision-makers on the design of programs like the APSS-CRDS, which aim to improve access to specialists, the essential components for the design of these types of interventions, and how contextual factors may influence program implementation. Variability in program design is important to consider as it may influence anticipated effects, a next step for the research team. Results may also inform stakeholders should they wish to implement similar programs to increase access to specialized health services via primary care.
2016 年,加拿大魁北克省实施了一项计划,旨在改善对专科医疗服务的获取途径(Accès priorisé aux services spécialisés (APSS)),其中包括通过初级保健设立单一区域服务接入点(Centre de répartition des demandes de services (CRDS))来处理对这些服务的请求。家庭医生使用标准化表格填写并提交专家初始咨询请求,该表格根据列出的咨询原因设置了预定的优先级,然后将其发送到集中转诊系统(CRDS),在该系统中为专家咨询分配。我们 1)使用逻辑模型描述了魁北克三个地区的 APSS-CRDS 计划;2)比较了 APSS-CRDS 模型的组件和流程的相似点和不同点;3)探讨了影响模型相似点和不同点的背景因素。
我们依靠一项定性研究,为三个地区实施的 APSS-CRDS 计划开发逻辑模型。对 9 名卫生行政管理人员进行了半结构化访谈。访谈采用框架分析方法进行分析,依据的是最初设计的方案中包含的 APSS-CRDS 组件、Mitchell 和 Lewis(2003)的逻辑模型框架以及 Chaudoir 及其同事(2013)关于背景因素对创新实施影响的框架。
研究结果表明,APSS-CRDS 计划在实施其组件方面存在区域差异,包括其结构(集中式/分散式)、实施和运营所涉及的人力资源、获取专家可用性和评估/转达请求的流程以及监测方法。差异可能是由背景因素的影响造成的,如部长级和医学协会的参与、合作、实施准备情况、医生实践特征以及计划的适应性。
研究结果有助于为决策者提供有关 APSS-CRDS 等计划的设计信息,这些计划旨在改善对专科医生的获取途径,这些计划的基本设计组件以及背景因素如何影响计划的实施。考虑计划设计的差异很重要,因为它可能会影响预期效果,这是研究团队的下一步工作。研究结果还可以为希望通过初级保健增加专科医疗服务获取途径的利益相关者提供信息。