Flores Raja, Patel Parth, Alpert Naomi, Pyenson Bruce, Taioli Emanuela
Department of Thoracic Surgery, Icahn School of Medicine at Mount Sinai, Mount Sinai Health System, New York, New York.
Institute for Translational Epidemiology and Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York, New York.
JAMA Netw Open. 2021 Dec 1;4(12):e2137508. doi: 10.1001/jamanetworkopen.2021.37508.
Early detection by computed tomography and a more attention-oriented approach to incidentally identified pulmonary nodules in the last decade has led to population stage shift for non-small cell lung cancer (NSCLC). This stage shift could substantially confound the evaluation of newer therapeutics and mortality outcomes.
To investigate the association of stage shift with population mortality among patients with NSCLC.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study was performed from October 2020 to June 2021 and used data from the Surveillance, Epidemiology, and End Results (SEER) registries to assess all patients from 2006 to 2016 with NSCLC.
Incidence-based mortality was evaluated by year-of-death. To assess shifts in diagnostic characteristics, clinical stage and histology distributions were examined by year using χ2 tests. Trends were assessed using the average annual percentage change (AAPC), calculated with JoinPoint software. Kaplan-Meier survival analysis assessed overall survival according to stage and compared those missing any stage with those with a reported stage.
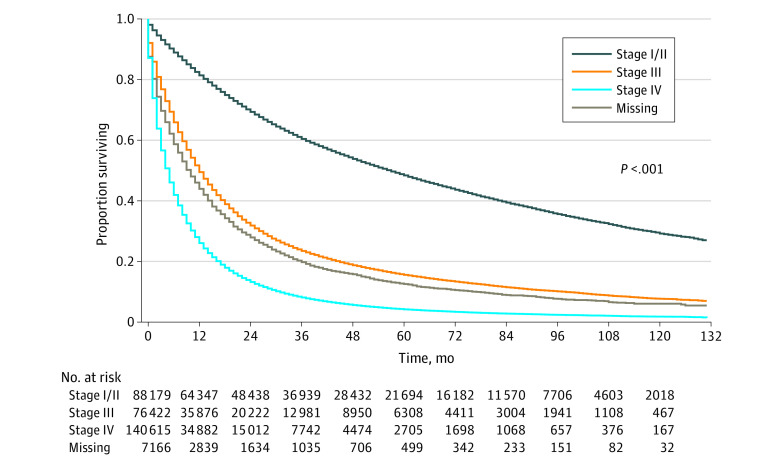
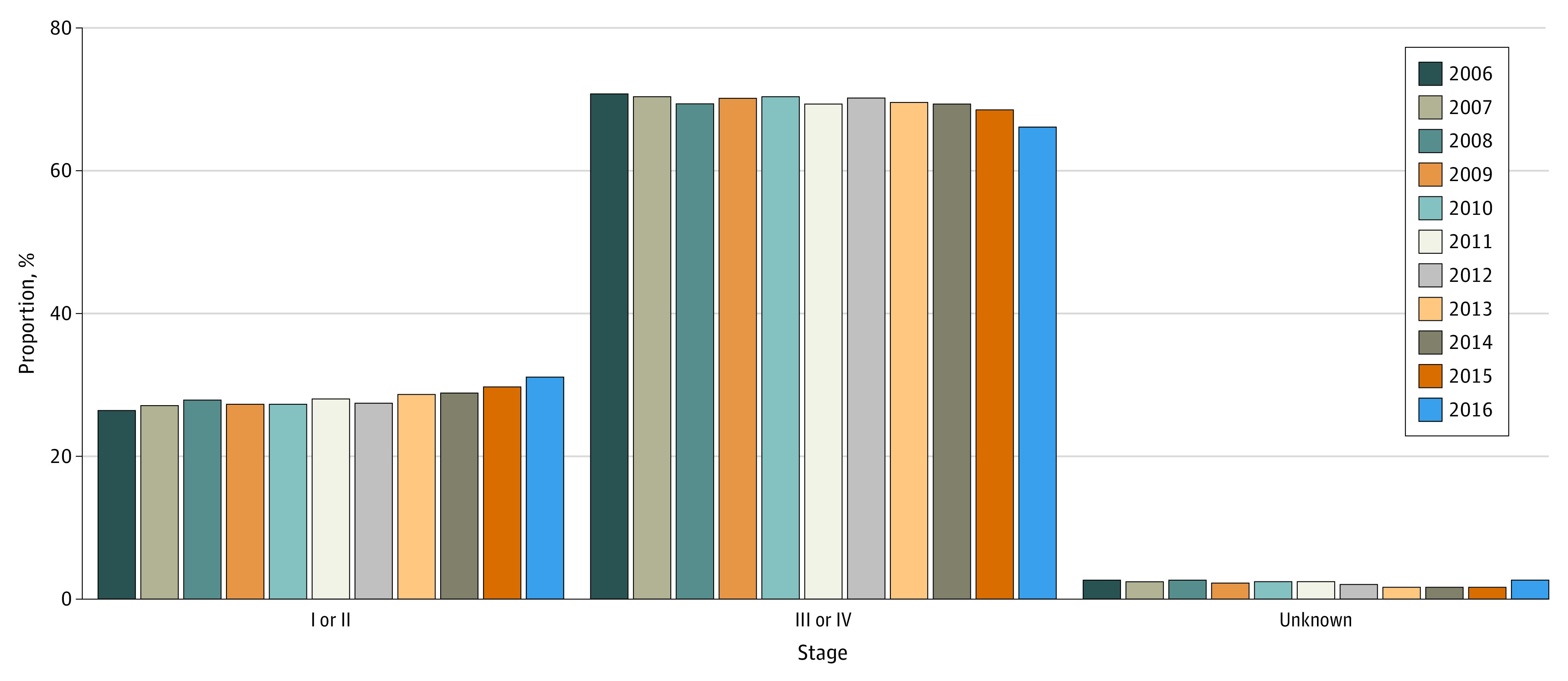
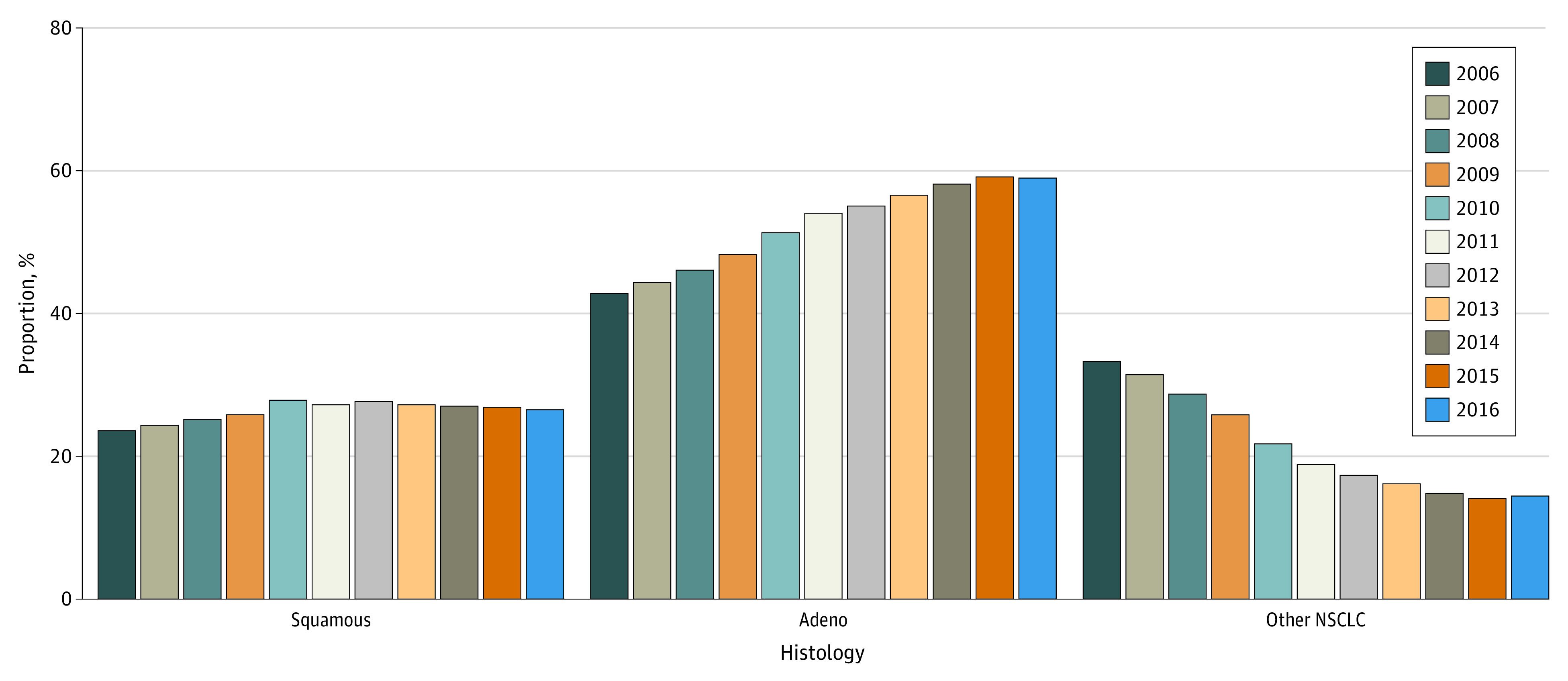
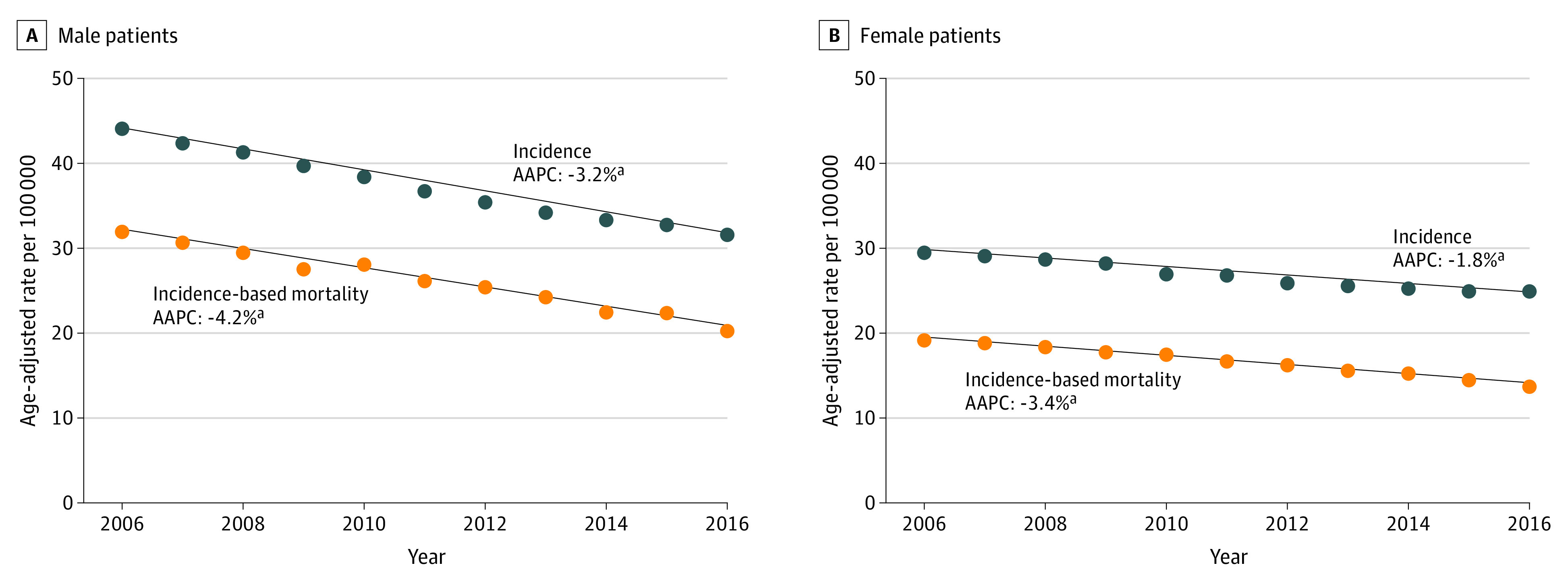
The final sample contained 312 382 patients; 166 657 (53.4%) were male, 38 201 (12.2%) were Black, and 249 062 (79.7%) were White; the median (IQR) age was 68 (60-76) years; 163 086 (52.2%) had adenocarcinoma histology. Incidence-based mortality within 5 years of diagnosis decreased from 2006 to 2016 (AAPC, -3.7; 95% CI, -4.1 to -3.4). When assessing stage shift, there was significant association between year-of-diagnosis and clinical stage, with stage I/II diagnosis increasing from 26.5% to 31.2% (AAPC, 1.5; 95% CI, 0.5 to 2.5); and stage III/IV diagnosis decreasing significantly from 70.8% to 66.1% (AAPC, -0.6; 95% CI, -1.0 to -0.2). Missing staging information was not associated with year-of-diagnosis (AAPC, -1.6; 95% CI, -7.4 to 4.5). Year-of-diagnosis was significantly associated with tumor histology (χ2 = 8990.0; P < .001). There was a significant increase in adenocarcinomas: 42.9% in 2006 to 59.0% in 2016 (AAPC, 3.4; 95% CI, 2.9 to 3.9). Median (IQR) survival for stage I/II was 57 months (18 months to not reached); stage III/IV was 7 (2-19) months; and missing stage was 10 (2-28) months. When compared with those with known stage, those without stage information had significantly worse survival than those with stage I/II, with survival between those with stage III and stage IV (log-rank χ2 = 87 125.0; P < .001).
This cohort study found an association between decreased mortality and a corresponding diagnostic shift from later to earlier stage. These findings suggest that studies investigating the effect of treatment on lung cancer must take into account stage shift and the confounding association with survival and mortality outcome.
在过去十年中,通过计算机断层扫描进行早期检测以及对偶然发现的肺结节采取更注重关注的方法,导致了非小细胞肺癌(NSCLC)的人群分期转变。这种分期转变可能会严重混淆对新型疗法和死亡率结果的评估。
研究NSCLC患者分期转变与人群死亡率之间的关联。
设计、设置和参与者:这项回顾性队列研究于2020年10月至2021年6月进行,使用监测、流行病学和最终结果(SEER)登记处的数据来评估2006年至2016年所有NSCLC患者。
根据死亡年份评估基于发病率的死亡率。为了评估诊断特征的变化,使用χ2检验按年份检查临床分期和组织学分布。使用JoinPoint软件计算的平均年度百分比变化(AAPC)评估趋势。Kaplan-Meier生存分析根据分期评估总生存,并将任何分期缺失的患者与有报告分期的患者进行比较。
最终样本包含312382名患者;166657名(53.4%)为男性,38201名(12.2%)为黑人,249062名(79.7%)为白人;中位(IQR)年龄为68(60 - 76)岁;163086名(52.2%)具有腺癌组织学。诊断后5年内基于发病率的死亡率从2006年到2016年有所下降(AAPC,-3.7;95%CI,-4.1至-3.4)。在评估分期转变时,诊断年份与临床分期之间存在显著关联,I/II期诊断从26.5%增加到31.2%(AAPC,1.5;95%CI,0.5至2.5);III/IV期诊断从70.8%显著下降到66.1%(AAPC,-0.6;95%CI,-1.0至-0.2)。分期信息缺失与诊断年份无关(AAPC,-1.6;95%CI,-7.4至4.5)。诊断年份与肿瘤组织学显著相关(χ2 = 8990.0;P <.001)。腺癌有显著增加:从2006年的42.9%增加到2016年的59.0%(AAPC,3.4;95%CI,2.9至3.9)。I/II期的中位(IQR)生存时间为57个月(18个月至未达到);III/IV期为7(2 - 19)个月;分期缺失为10(2 - 28)个月。与有已知分期的患者相比,无分期信息的患者生存情况明显差于I/II期患者,生存情况介于III期和IV期患者之间(对数秩χ2 = 87125.0;P <.001)。
这项队列研究发现死亡率降低与相应的从晚期到早期的诊断转变之间存在关联。这些发现表明,研究治疗对肺癌影响的研究必须考虑分期转变以及与生存和死亡率结果的混淆关联。