Piersma F R, Neefs J, Berger W R, van den Berg N W E, Wesselink R, Krul S P J, de Groot J R
Department of Cardiology, Heart Centre, Amsterdam University Medical Centres, University of Amsterdam, Amsterdam, The Netherlands.
Neth Heart J. 2022 Jul;30(7-8):370-376. doi: 10.1007/s12471-021-01651-x. Epub 2021 Dec 17.
Atrial fibrillation (AF) is the most common arrhythmia and imposes a high burden on the healthcare system. A nurse-led AF outpatient clinic may alleviate the burden on the cardiology outpatient clinic by triaging patients who need care by a cardiologist or general practitioner (GP). However, care and referral patterns after initial assessment in a nurse-led AF outpatient clinic are unknown. We examined the proportion of AF patients assessed in a nurse-led clinic without outpatient follow-up by a cardiologist.
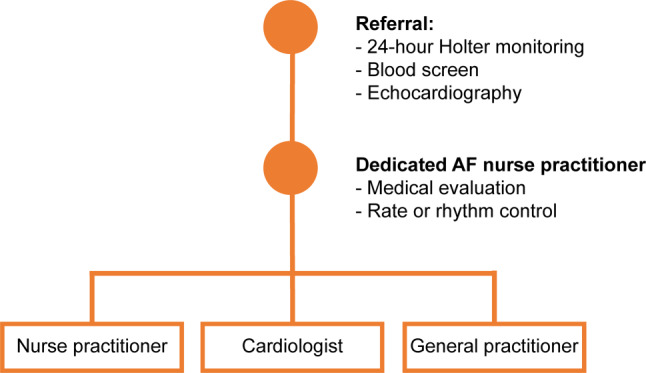
All patients with AF referred to our tertiary medical centre underwent cardiac work-up in the nurse-led AF outpatient clinic and were prospectively followed. Data on patient characteristics, rhythm monitoring and echocardiography were collected and described. Odds ratio (OR) for continuing care in the nurse-led AF outpatient clinic was calculated.
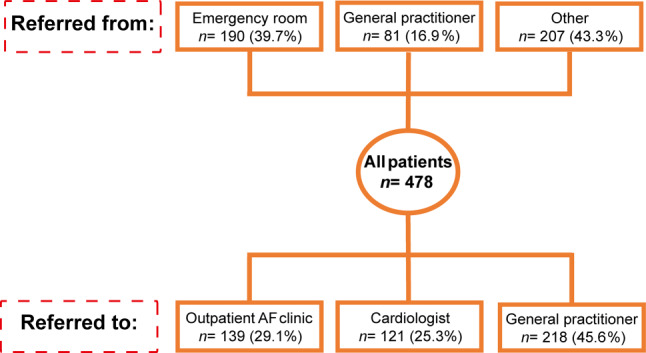
From 2014 to 2018, 478 consecutive individual patients were referred to the nurse-led AF outpatient clinic. After the initial cardiac work-up, 139 patients (29.1%) remained under nurse-led care and 121 (25.3%) were referred to a cardiologist and 218 (45.6%) to a GP. Patients who remained under nurse-led care were significantly younger, were more symptomatic, more often had paroxysmal AF and had less comorbidities than the other two groups. After multivariable testing, CHADS-VASc score ≥ 2 was associated with discontinued nurse-led care (OR 0.57, 95% confidence interval 0.34-0.95).
After initial cardiac assessment in the nurse-led outpatient clinic, about half of the newly referred AF patients were referred back to their GP. This strategy may reduce the burden of AF patients on secondary or tertiary cardiology outpatient clinics.
心房颤动(AF)是最常见的心律失常,给医疗系统带来了沉重负担。由护士主导的房颤门诊可以通过对需要心脏病专家或全科医生(GP)护理的患者进行分诊,减轻心脏病门诊的负担。然而,在由护士主导的房颤门诊进行初步评估后的护理和转诊模式尚不清楚。我们研究了在由护士主导的诊所接受评估且未由心脏病专家进行门诊随访的房颤患者比例。
所有转诊至我们三级医疗中心的房颤患者在由护士主导的房颤门诊接受心脏检查,并进行前瞻性随访。收集并描述了患者特征、心律监测和超声心动图的数据。计算了在由护士主导的房颤门诊继续护理的比值比(OR)。
2014年至2018年,478例连续个体患者被转诊至由护士主导的房颤门诊。在初步心脏检查后,139例患者(29.1%)仍由护士主导护理,121例(25.3%)被转诊至心脏病专家处,218例(45.6%)被转诊至全科医生处。与其他两组相比,仍由护士主导护理的患者明显更年轻、症状更明显、阵发性房颤更常见且合并症更少。经过多变量测试,CHADS-VASc评分≥2与停止由护士主导的护理相关(OR 0.57,95%置信区间0.34-0.95)。
在由护士主导的门诊进行初步心脏评估后,约一半新转诊的房颤患者被转回其全科医生处。这种策略可能会减轻房颤患者对二级或三级心脏病门诊的负担。