Division of Infectious Diseases and International Health, Department of Medicine, Duke University, Durham, North Carolina.
Duke Global Health Institute, Duke University, Durham, North Carolina.
Am J Trop Med Hyg. 2021 Dec 20;106(2):494-503. doi: 10.4269/ajtmh.20-1036.
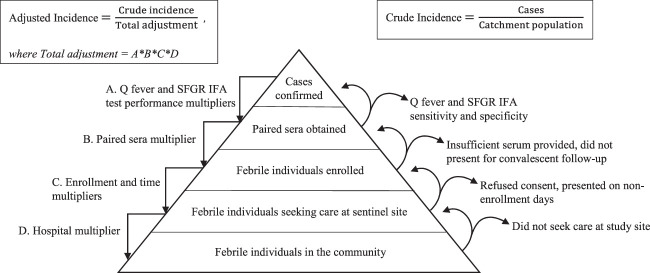
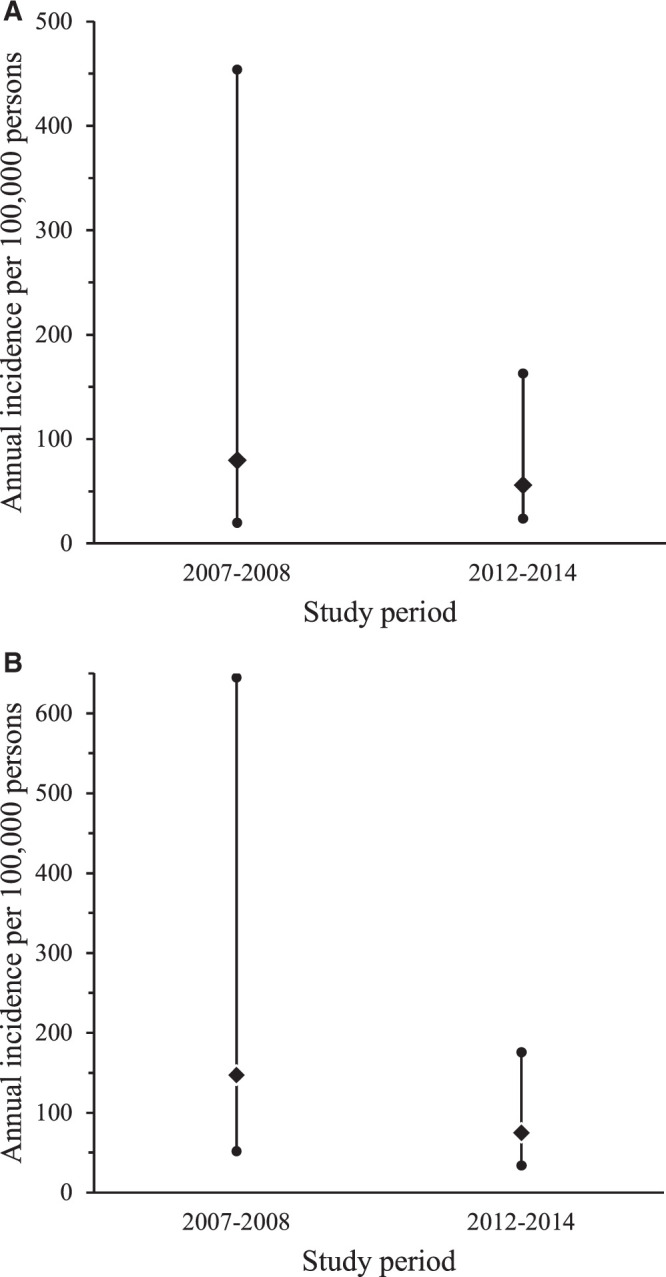
Q fever and spotted fever group rickettsioses (SFGR) are common causes of severe febrile illness in northern Tanzania. Incidence estimates are needed to characterize the disease burden. Using hybrid surveillance-coupling case-finding at two referral hospitals and healthcare utilization data-we estimated the incidences of acute Q fever and SFGR in Moshi, Kilimanjaro, Tanzania, from 2007 to 2008 and from 2012 to 2014. Cases were defined as fever and a four-fold or greater increase in antibody titers of acute and convalescent paired sera according to the indirect immunofluorescence assay of Coxiella burnetii phase II antigen for acute Q fever and Rickettsia conorii (2007-2008) or Rickettsia africae (2012-2014) antigens for SFGR. Healthcare utilization data were used to adjust for underascertainment of cases by sentinel surveillance. For 2007 to 2008, among 589 febrile participants, 16 (4.7%) of 344 and 27 (8.8%) of 307 participants with paired serology had Q fever and SFGR, respectively. Adjusted annual incidence estimates of Q fever and SFGR were 80 (uncertainty range, 20-454) and 147 (uncertainty range, 52-645) per 100,000 persons, respectively. For 2012 to 2014, among 1,114 febrile participants, 52 (8.1%) and 57 (8.9%) of 641 participants with paired serology had Q fever and SFGR, respectively. Adjusted annual incidence estimates of Q fever and SFGR were 56 (uncertainty range, 24-163) and 75 (uncertainty range, 34-176) per 100,000 persons, respectively. We found substantial incidences of acute Q fever and SFGR in northern Tanzania during both study periods. To our knowledge, these are the first incidence estimates of either disease in sub-Saharan Africa. Our findings suggest that control measures for these infections warrant consideration.
在坦桑尼亚北部,Q 热和斑点热群立克次体(SFGR)是引起严重发热疾病的常见原因。需要发病率估计来描述疾病负担。本研究通过在两家转诊医院进行混合监测-病例发现和医疗保健利用数据,估计了 2007 年至 2008 年和 2012 年至 2014 年坦桑尼亚莫希、乞力马扎罗地区急性 Q 热和 SFGR 的发病率。病例定义为发热和根据间接免疫荧光分析柯克斯体二期抗原的急性和恢复期配对血清的四倍或以上滴度增加,用于急性 Q 热和立氏立克次体(2007-2008 年)或非洲立克次体(2012-2014 年)抗原的 SFGR。利用医疗保健利用数据来调整哨点监测中病例的漏报。2007 年至 2008 年,在 589 名发热参与者中,344 名参与者中有 16 名(4.7%)和 307 名参与者中有 27 名(8.8%)的配对血清学检查结果为 Q 热和 SFGR。调整后的急性 Q 热和 SFGR 发病率估计分别为每 100,000 人 80(不确定性范围,20-454)和 147(不确定性范围,52-645)。2012 年至 2014 年,在 1114 名发热参与者中,641 名参与者中有 52 名(8.1%)和 57 名(8.9%)的配对血清学检查结果为 Q 热和 SFGR。调整后的急性 Q 热和 SFGR 发病率估计分别为每 100,000 人 56(不确定性范围,24-163)和 75(不确定性范围,34-176)。我们在两个研究期间都发现了大量的急性 Q 热和 SFGR 发病率。据我们所知,这是撒哈拉以南非洲地区首次对这两种疾病进行发病率估计。我们的研究结果表明,这些感染的控制措施值得考虑。