Department of Surgery, Massachusetts General Hospital, Harvard Medical School, Boston.
JAMA Oncol. 2022 Mar 1;8(3):462-473. doi: 10.1001/jamaoncol.2021.5970.
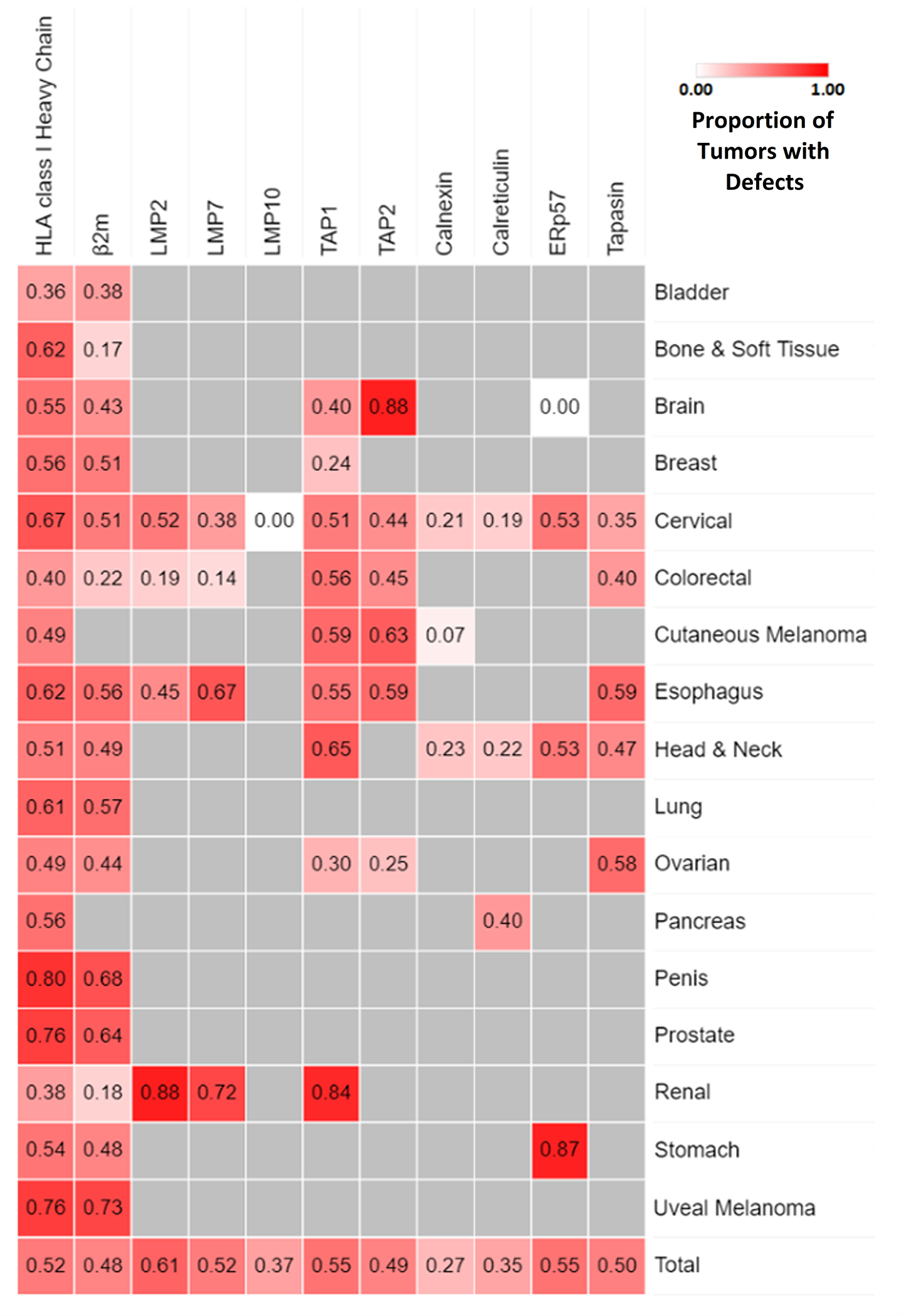
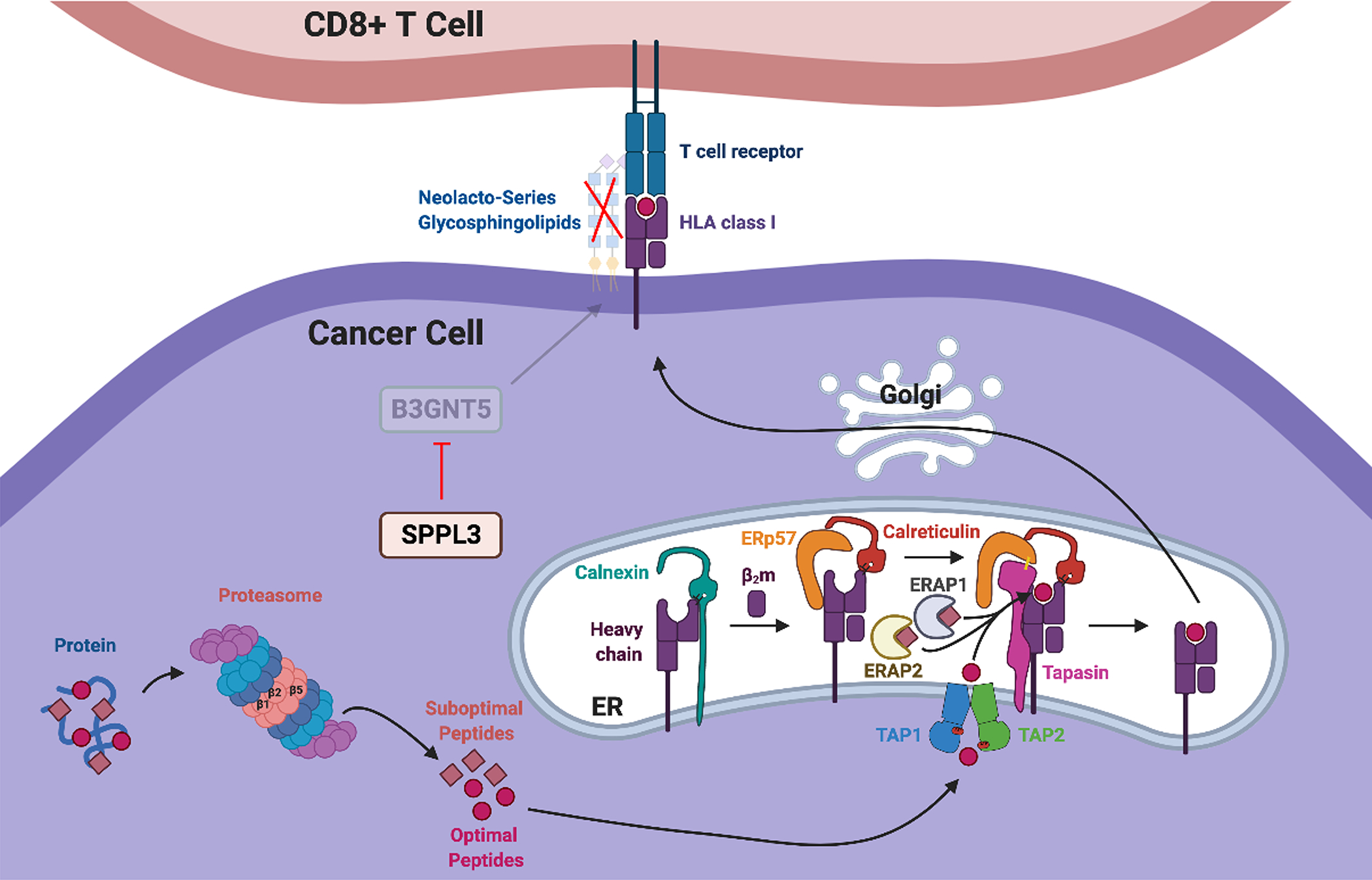
Although typically impressive, objective responses to immune checkpoint inhibitors (ICIs) occur in only 12.5% of patients with advanced cancer. The majority of patients do not respond due to cell-intrinsic resistance mechanisms, including human leukocyte antigen (HLA) class I antigen-processing machinery (APM) defects. The APM defects, which have a negative effect on neoantigen presentation to cytotoxic T lymphocytes (CTLs), are present in the majority of malignant tumors. These defects are caused by gene variations in less than 25% of cases and by dysregulated signaling and/or epigenetic changes in most of the remaining cases, making them frequently correctable. This narrative review summarizes the growing clinical evidence that chemotherapy, targeted therapies, and, to a lesser extent, radiotherapy can correct HLA class I APM defects in cancer cells and improve responses to ICIs.
Most chemotherapeutics enhance HLA class I APM component expression and function in cancer cells, tumor CTL infiltration, and responses to ICIs in preclinical and clinical models. Despite preclinical evidence, radiotherapy does not appear to upregulate HLA class I expression in patients and does not enhance the efficacy of ICIs in clinical settings. The latter findings underscore the need to optimize the dose and schedule of radiation and timing of ICI administration to maximize their immunogenic synergy. By increasing DNA and chromatin accessibility, epigenetic agents (histone deacetylase inhibitors, DNA methyltransferase inhibitors, and EZH2 inhibitors) enhance HLA class I APM component expression and function in many cancer types, a crucial contributor to their synergy with ICIs in patients. Furthermore, epidermal growth factor receptor (EGFR) inhibitors and BRAF/mitogen-activated protein kinase kinase inhibitors are effective at upregulating HLA class I expression in EGFR- and BRAF-variant tumors, respectively; these changes may contribute to the clinical responses induced by these inhibitors in combination with ICIs.
This narrative review summarizes evidence indicating that chemotherapy and targeted therapies are effective at enhancing HLA class I APM component expression and function in cancer cells. The resulting increased immunogenicity and recognition and elimination of cancer cells by cognate CTLs contributes to the antitumor activity of these therapies as well as to their synergy with ICIs.
尽管免疫检查点抑制剂(ICIs)通常能产生令人印象深刻的效果,但只有 12.5%的晚期癌症患者出现客观应答。由于细胞内在的耐药机制,大多数患者无法应答,包括人类白细胞抗原(HLA)I 类抗原加工机制(APM)缺陷。APM 缺陷对细胞毒性 T 淋巴细胞(CTL)的新抗原呈递有负面影响,存在于大多数恶性肿瘤中。这些缺陷在不到 25%的病例中是由基因突变引起的,在大多数剩余病例中是由信号失调和/或表观遗传变化引起的,因此经常是可以纠正的。这篇叙述性综述总结了越来越多的临床证据,表明化疗、靶向治疗,在较小程度上还有放疗,可以纠正癌细胞中的 HLA I 类 APM 缺陷,并改善对 ICI 的应答。
大多数化疗药物可增强癌细胞、肿瘤 CTL 浸润以及临床前和临床模型中对 ICI 的应答中的 HLA I 类 APM 成分的表达和功能。尽管有临床前证据,但放疗似乎不会上调患者的 HLA I 类表达,也不会增强 ICI 在临床环境中的疗效。后一种发现强调需要优化放疗的剂量和方案以及 ICI 给药的时间,以最大限度地发挥它们的免疫协同作用。通过增加 DNA 和染色质的可及性,表观遗传药物(组蛋白去乙酰化酶抑制剂、DNA 甲基转移酶抑制剂和 EZH2 抑制剂)可增强许多癌症类型中的 HLA I 类 APM 成分的表达和功能,这是它们与患者的 ICI 协同作用的关键贡献。此外,表皮生长因子受体(EGFR)抑制剂和 BRAF/丝裂原激活蛋白激酶激酶抑制剂分别有效地上调 EGFR 和 BRAF 变异肿瘤中的 HLA I 类表达;这些变化可能有助于这些抑制剂与 ICI 联合诱导的临床应答。
这篇叙述性综述总结了表明化疗和靶向治疗可有效增强癌细胞中 HLA I 类 APM 成分表达和功能的证据。由此增加的免疫原性以及同源 CTL 对癌细胞的识别和消除有助于这些疗法的抗肿瘤活性以及它们与 ICI 的协同作用。