Cho Eun-Ju, Jung Gu-Cheol, Kwak Min-Sun, Yang Jong-In, Yim Jeong-Yoon, Yu Su-Jong, Chung Goh-Eun
Department of Internal Medicine and Liver Research Institute, Seoul National University College of Medicine, Seoul 03080, Korea.
Healthcare Research Institute, Gangnam Healthcare Center, Seoul National University Hospital, Seoul 06236, Korea.
Diagnostics (Basel). 2021 Nov 29;11(12):2233. doi: 10.3390/diagnostics11122233.
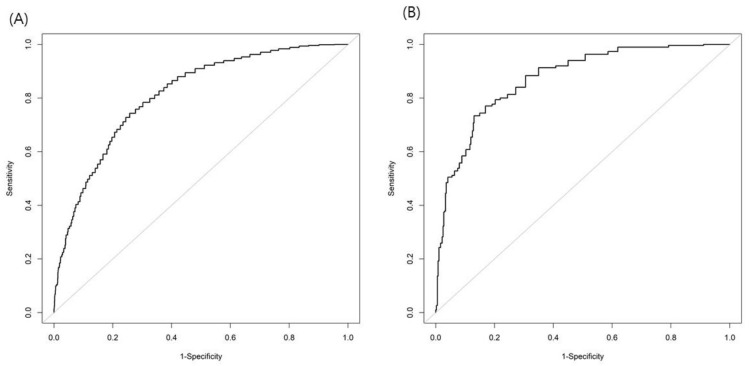
Nonalcoholic fatty liver disease (NAFLD) is increasing worldwide, highlighting the importance of early and accurate detection and the appropriate management of NAFLD. However, ultrasonography (US) is not included in many mass screening programs, and people have limited access to it. The aim of this study is to validate the fatty liver index (FLI) and investigate the optimal cutoff value for predicting NAFLD in an asymptomatic population. We conducted a retrospective cohort study in Korea. All subjects who underwent health checkup exams, including abdominal US, controlled attenuation parameter (CAP) and blood testing, were enrolled. Analyses of the area under the receiver operating characteristic curve (AUROC) were used to evaluate the diagnostic accuracy and to calculate the optimal FLI cutoff for US-NAFLD. Among the 4009 subjects (mean age 54.9 years, 83.5% male), the prevalence of US-diagnosed NAFLD and CAP-defined hepatic steatosis was 61.4% and 55.4%. The previously used cutoff of FLI = 60 showed poor performance in predicting US-diagnosed NAFLD, with an AUROC of 0.63 (0.62-0.64), and CAP-defined NAFLD, with an AUROC 0.63 (0.62-0.64). The optimal FLI cutoff values to discriminate fatty liver detected by US were 29 for the entire population, with an AUROC of 0.82 (0.81-0.84). The sex-specific values were 31 for males and 18 for females (sensitivity 72.8% and 73.4%; specificity 74.2% and 85.0%, respectively). The FLI cutoff for US-diagnosed NAFLD can be set as 29 for the entire Korean population. Considering the sex dimorphism in NAFLD, different cutoff values are suggested to predict US-diagnosed NAFLD. These results may be helpful in the accurate non-invasive diagnosis of NAFLD.
非酒精性脂肪性肝病(NAFLD)在全球范围内呈上升趋势,凸显了早期准确检测及对NAFLD进行适当管理的重要性。然而,许多大规模筛查项目并未将超声检查(US)纳入其中,人们进行超声检查的机会有限。本研究的目的是验证脂肪肝指数(FLI),并探讨在无症状人群中预测NAFLD的最佳临界值。我们在韩国进行了一项回顾性队列研究。纳入所有接受了包括腹部超声、受控衰减参数(CAP)和血液检测在内的健康体检的受试者。采用受试者操作特征曲线下面积(AUROC)分析来评估诊断准确性,并计算US-NAFLD的最佳FLI临界值。在4009名受试者(平均年龄54.9岁,83.5%为男性)中,超声诊断的NAFLD患病率和CAP定义的肝脂肪变性患病率分别为61.4%和55.4%。先前使用的FLI = 60的临界值在预测超声诊断的NAFLD方面表现不佳,AUROC为0.63(0.62 - 0.64),在预测CAP定义的NAFLD方面,AUROC为0.63(0.62 - 0.64)。区分超声检测到的脂肪肝的最佳FLI临界值在总体人群中为29,AUROC为0.82(0.81 - 0.84)。按性别划分的值,男性为31,女性为18(敏感性分别为72.8%和73.4%;特异性分别为74.2%和85.0%)。对于整个韩国人群,超声诊断的NAFLD的FLI临界值可设定为29。考虑到NAFLD中的性别差异,建议采用不同的临界值来预测超声诊断的NAFLD。这些结果可能有助于NAFLD的准确无创诊断。