Pneumology, Centre Hospitalier Du Mans, Le Mans, France.
Cancer Medicine Department, Gustave Roussy, Villejuif, France; Paris-Saclay University, Orsay, France.
ESMO Open. 2022 Feb;7(1):100353. doi: 10.1016/j.esmoop.2021.100353. Epub 2021 Dec 23.
Immunotherapy using inhibitors targeting immune checkpoint programmed cell death protein 1 (PD-1)/programmed death-ligand 1 (PD-L1) is currently the standard of care in patients with advanced non-small-cell lung cancer (NSCLC).
We carried out a nationwide cohort retrospective study of consecutive patients with advanced, refractory NSCLC who received nivolumab as second to later lines of treatment as part of the expanded access program. Key objectives were to assess the efficacy and safety of nivolumab and the efficacy of first post-nivolumab treatment.
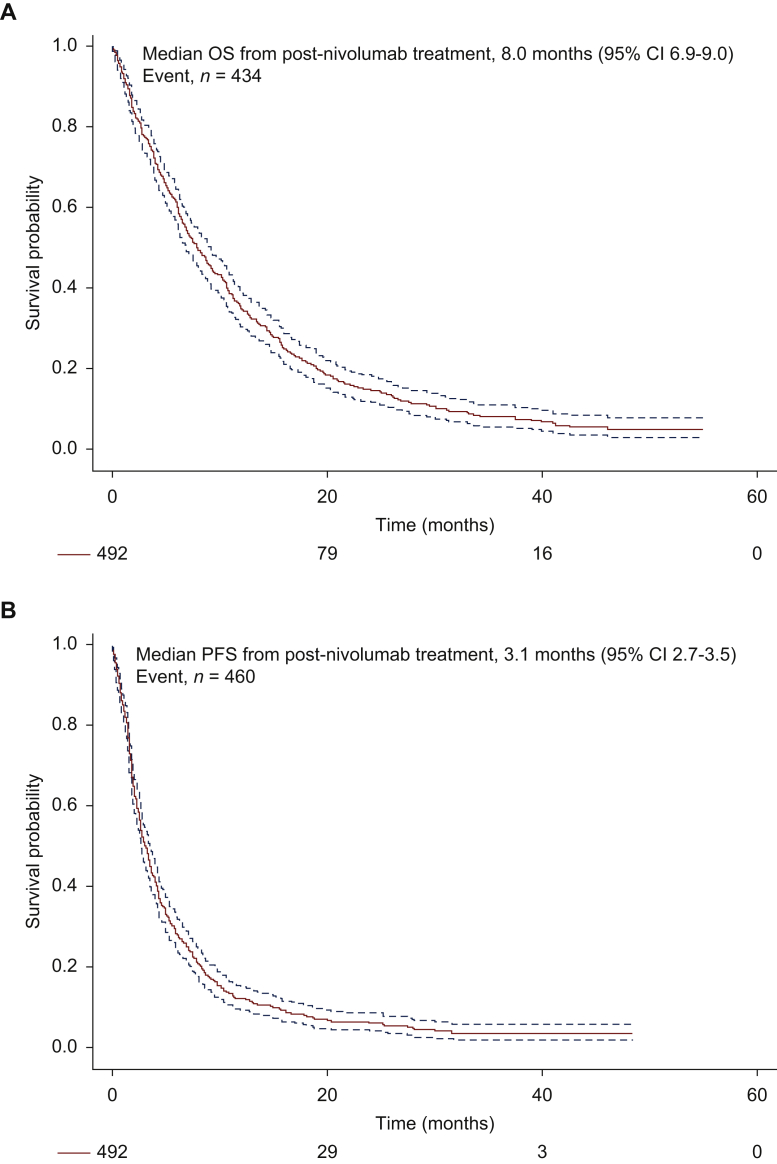
Nine hundred and two patients were enrolled: 317 (35%) with squamous cell carcinoma and 585 (65%) with non-squamous cell carcinoma. Median age was 64 years; there were 630 (70%) men, 795 (88%) smokers, 723 (81%) patients with an Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0/1, 197 (22%) patients with brain metastases, and 212 (27%) with liver metastases. Best response was partial response for 16.2% and stable disease (SD) for 30.5%. Progression-free survival and overall survival (OS) rates at 2, 3, and 5 years were 8% and 25%, 6% and 16%, and 4% and 10%, respectively. At multivariate analysis, ECOG PS ≥2 [hazard ratio (HR) = 2.13, 95% confidence interval (95% CI) 1.78-2.55, P < 0.001], squamous histology (HR = 1.17, 95% CI 1.01-1.36, P = 0.04), and presence of central nervous system metastases (HR = 1.29, 95% CI 1.08-1.54, P = 0.005) were significantly associated with lower OS. Four hundred and ninety-two patients received at least one treatment after discontinuation of nivolumab, consisting of systemic therapies in 450 (91%). Radiation therapy was delivered to 118 (24%) patients.
The CLINIVO cohort represents the largest real-world evidence cohort with the use of immune checkpoint inhibitor in advanced, metastatic NSCLC after failure of first-line chemotherapy, with long-term follow-up and analysis of subsequent therapies. Our data confirm the efficacy of nivolumab in a cohort larger than that reported in landmark clinical trials and identify prognostic factors, which reinforces the need for accurate selection of patients for treatment with immune checkpoint inhibitors. Our data indicate that oligoprogression is frequent after nivolumab exposure and provide a unique insight into the long-term survival.
免疫疗法使用针对免疫检查点程序性细胞死亡蛋白 1(PD-1)/程序性死亡配体 1(PD-L1)的抑制剂,目前是晚期非小细胞肺癌(NSCLC)患者的标准治疗方法。
我们对接受纳武利尤单抗二线及后线治疗的晚期难治性 NSCLC 连续患者进行了全国性队列回顾性研究,该研究纳入患者是参与扩展准入计划的患者。主要目的是评估纳武利尤单抗的疗效和安全性,以及首次纳武利尤单抗治疗后的疗效。
共纳入 902 例患者:317 例(35%)为鳞状细胞癌,585 例(65%)为非鳞状细胞癌。中位年龄为 64 岁;630 例(70%)为男性,795 例(88%)为吸烟者,723 例(81%)患者的东部肿瘤协作组(ECOG)体能状态(PS)为 0/1,197 例(22%)患者有脑转移,212 例(27%)有肝转移。最佳缓解为部分缓解(16.2%)和疾病稳定(SD)(30.5%)。2、3、5 年无进展生存率和总生存率(OS)分别为 8%和 25%、6%和 16%、4%和 10%。多变量分析显示,ECOG PS ≥2(风险比[HR]2.13,95%置信区间[95%CI]1.78-2.55,P<0.001)、鳞状组织学(HR 1.17,95%CI 1.01-1.36,P=0.04)和存在中枢神经系统转移(HR 1.29,95%CI 1.08-1.54,P=0.005)与较低的 OS 显著相关。492 例患者在停用纳武利尤单抗后至少接受了一种治疗,其中 450 例(91%)接受了系统治疗。118 例(24%)患者接受了放射治疗。
CLINIVO 队列是最大的真实世界证据队列,使用免疫检查点抑制剂治疗一线化疗失败后的晚期转移性 NSCLC,具有长期随访和后续治疗分析。我们的数据证实了纳武利尤单抗在大于临床试验报告的队列中的疗效,并确定了预后因素,这再次强调了为免疫检查点抑制剂治疗选择准确患者的必要性。我们的数据表明,纳武利尤单抗暴露后常出现寡进展,为长期生存提供了独特的见解。