Néphrologie et Dialyse, Centre Hospitalier Le Mans, 194 Avenue Rubillard, 72037 Le Mans, France.
Nutrients. 2021 Dec 6;13(12):4371. doi: 10.3390/nu13124371.
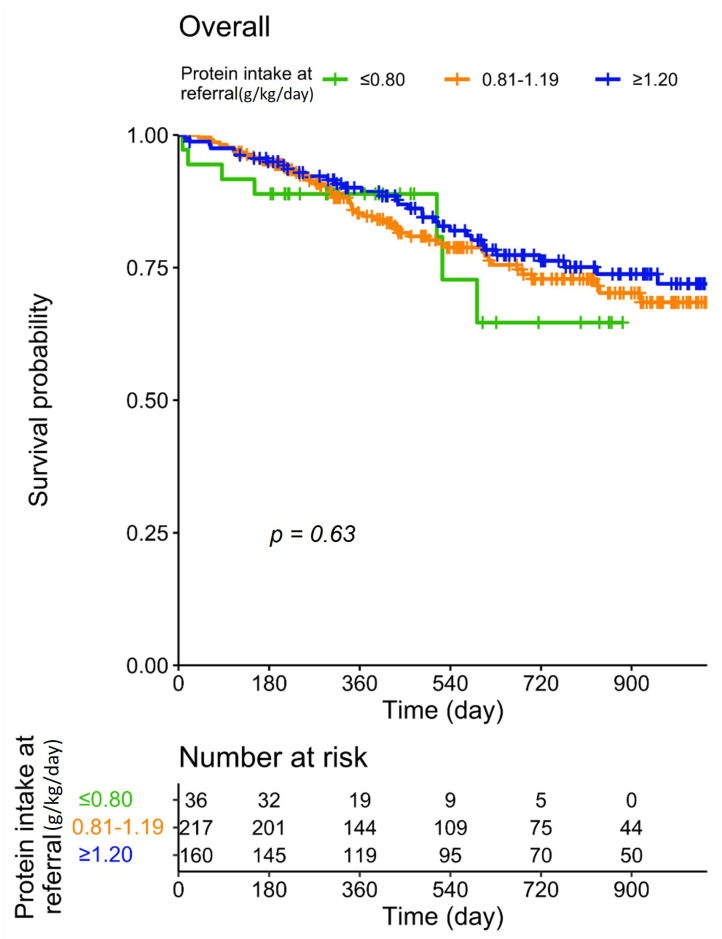
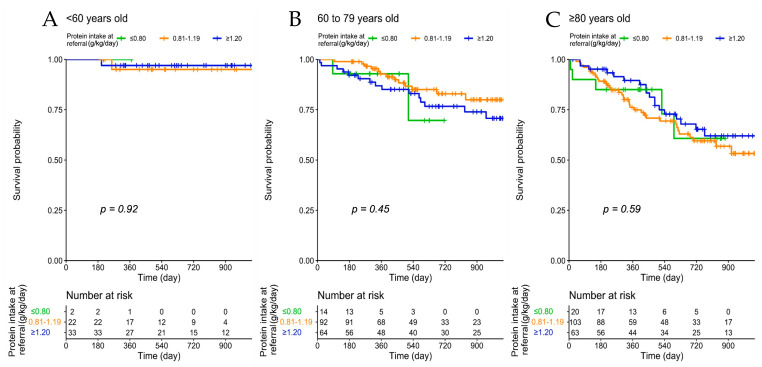
The recent guidelines on nutritional management of chronic kidney disease (CKD) advise a reduction in protein intake as early as CKD stage 3, regardless of age, to slow kidney function impairment. However, since elderly patients are usually considered as having a spontaneously reduced protein intake, nutritional interventions to reduce protein intake are often considered futile. This study aimed to assess the baseline protein intake of elderly CKD patients referred for nephrology care, and explore the need for dietary evaluations, focusing on the current recommendations for protein restriction in CKD. This is an observational study of CKD patients followed in the unit dedicated to advanced CKD patients in Le Mans, France. Patients with stages 3 to 5 not on dialysis were included. All patients were evaluated by an expert dietician to assess their baseline protein intake, whenever possible on the basis of a 7-days diet journal; when this was not available, dietary recall or analysis of delivered meals was employed. Demographic characteristics, underlying kidney disease, Charlson Comorbidity Index (CCI), Malnutrition-Inflammation Score (MIS), Subjective Global Assessment (SGA) and clinical and laboratory data were recorded. Between 15 November 2017 and 31 December 2020, 436 patients were evaluated in the unit. Their age distribution was as follows: "young": <60 ( = 62), "young-old": 60-69 ( = 74), "old": 70-79 ( = 108), "old-old": 80-89 ( = 140) and "oldest-old": ≥90 ( = 54). The prevalence of vascular nephropathies was higher in patients older than 70 years compared to younger ones, as did CCI and MIS ( < 0.001). Moderate nutritional impairment (SGA: B) was higher in elderly patients, reaching 53.7% at ≥90, while less than 3% of patients in the overall cohort were classified as SGA C ( < 0.001). The median protein intake was higher than the recommended one of 0.8 g/kg/day in all age groups; it was 1.2 g/kg/day in younger patients and 1.0 thereafter ( < 0.001). Patient survival depended significantly on age ( < 0.001) but not on baseline protein intake ( = 0.63), and younger patients were more likely to start dialysis during follow-up ( < 0.001). Over half of the patients, including the old-old and oldest-old, were still on follow-up two years after referral and it was found that survival was only significantly associated with age and comorbidity and was not affected by baseline protein intake. Our study shows that most elderly patients, including old-old and extremely old CKD patients, are spontaneously on diets whose protein content is higher than recommended, and indicates there is a need for nutritional care for this population.
最近关于慢性肾脏病(CKD)营养管理的指南建议,无论年龄大小,只要处于 CKD 第 3 期,就应减少蛋白质摄入,以减缓肾功能损害。然而,由于老年患者通常被认为蛋白质摄入自然减少,因此减少蛋白质摄入的营养干预通常被认为是徒劳的。本研究旨在评估接受肾病治疗的老年 CKD 患者的基线蛋白质摄入量,并探讨进行饮食评估的必要性,重点关注当前 CKD 蛋白质限制的建议。这是一项对法国勒芒专门为晚期 CKD 患者服务的单位中 CKD 患者进行的观察性研究。纳入了未接受透析的 3 至 5 期患者。所有患者均由专家营养师进行评估,尽可能根据 7 天饮食日记评估其基线蛋白质摄入量;当无法获得时,采用饮食回忆或分析已提供的膳食。记录了人口统计学特征、基础肾脏疾病、Charlson 合并症指数(CCI)、营养不良-炎症评分(MIS)、主观全面评估(SGA)以及临床和实验室数据。2017 年 11 月 15 日至 2020 年 12 月 31 日,该单位共评估了 436 名患者。他们的年龄分布如下:“年轻”<60(=62),“年轻老”60-69(=74),“老”70-79(=108),“年老”80-89(=140)和“最年老”≥90(=54)。与年轻患者相比,70 岁以上患者的血管性肾病患病率更高,CCI 和 MIS 也更高(<0.001)。营养中度受损(SGA:B)在老年患者中更为常见,≥90 岁时达到 53.7%,而整个队列中不到 3%的患者被归类为 SGA C(<0.001)。所有年龄组的蛋白质摄入量中位数均高于推荐的 0.8 g/kg/天;年轻患者为 1.2 g/kg/天,此后为 1.0 g/kg/天(<0.001)。患者的存活率与年龄显著相关(<0.001),但与基线蛋白质摄入无关(=0.63),且年轻患者在随访期间更有可能开始透析(<0.001)。超过一半的患者,包括年老和最年老的患者,在转诊后两年仍在接受随访,研究发现,存活率仅与年龄和合并症显著相关,不受基线蛋白质摄入的影响。我们的研究表明,大多数老年患者,包括年老和非常年老的 CKD 患者,其饮食中的蛋白质含量自然高于推荐量,这表明该人群需要进行营养护理。