Daneshpour Hediyeh, Brüdgam Denise, Stüfchen Isabel, Heinrich Daniel Alexander, Bidlingmaier Martin, Beuschlein Felix, Kürzinger Lydia, Williams Tracy Ann, Reincke Martin, Schneider Holger, Adolf Christian
Medizinische Klinik und Poliklinik IV, Klinikum der Universität München, Ludwig-Maximilians-Universität (LMU) München, Munich, Germany.
Klinik für Endokrinologie, Diabetologie und Klinische Ernährung, Universitätsspital Zürich (USZ) und Universität Zürich (UZH), Zurich, Switzerland.
Front Endocrinol (Lausanne). 2024 Nov 29;15:1495959. doi: 10.3389/fendo.2024.1495959. eCollection 2024.
Primary aldosteronism (PA) is the most common form of endocrine hypertension. According to the Endocrine Society Practice Guidelines, the diagnosis of PA requires a pathological screening test result and non-suppressible aldosterone levels during confirmatory testing. Sequential testing with more than one confirmatory test may result in discordant test results.
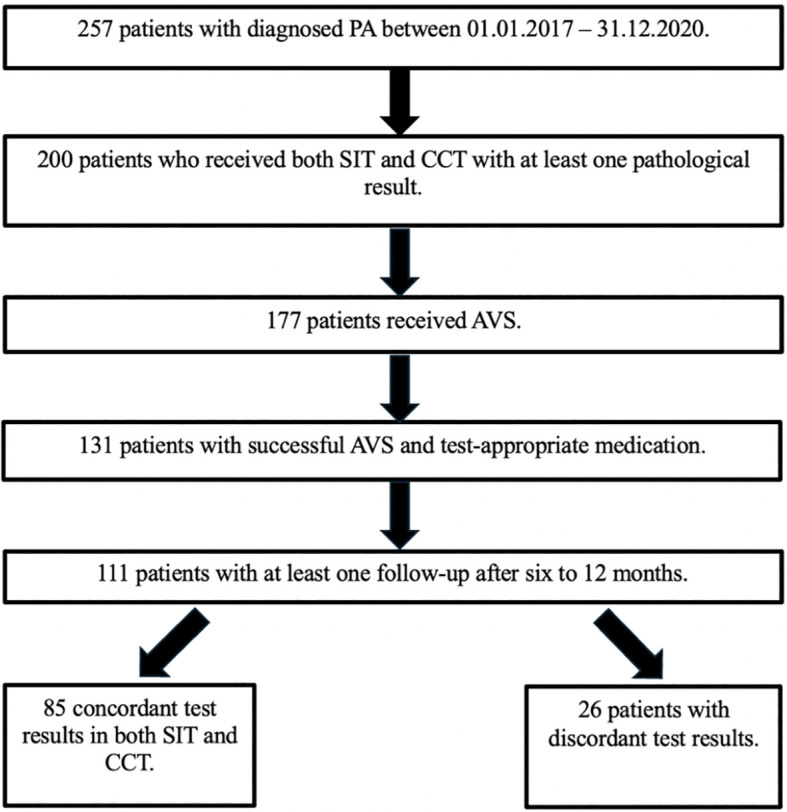
We investigated the association of discordant results of captopril challenge test (CCT) and saline infusion test (SIT) on patient subtype classification by adrenal vein sampling (AVS) and outcome in 111 consecutive patients from the German Conn's Registry. Concordance was defined as non-suppressible aldosterone levels upon both tests, while discordance was defined as conflicting test results. Patients with unilateral disease were offered adrenalectomy (ADX). Biochemical and clinical outcomes were assessed using the PASO criteria.
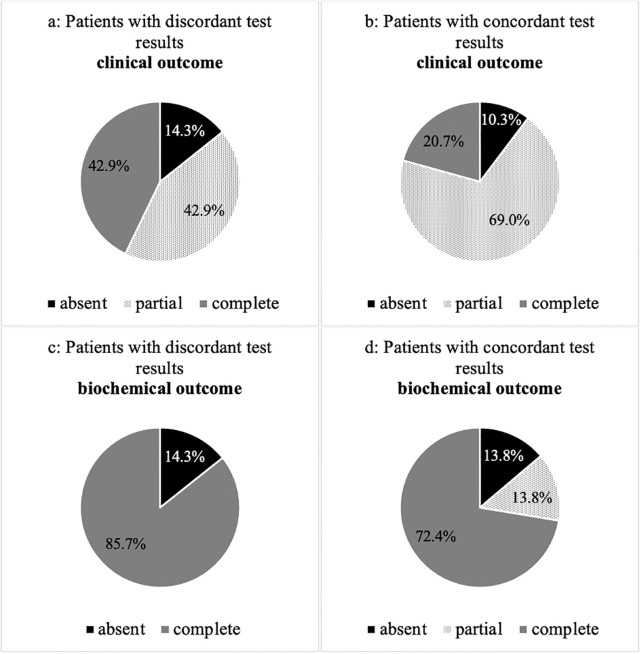
85 of 111 (77%) patients had concordant results of CCT and SIT. Although baseline characteristics were comparable between patients with concordant and discordant tests, the latter had significantly lower aldosterone levels after testing (CCT: 170 vs. 114pg/ml; SIT: 139 vs. 101pg/ml; p=0.004). In 35% of patients with discordant (n=9) and 46% of concordant test results (n=39), AVS suggested lateralized PA. In 36 of 48 cases ADX was performed. 86% of patients with discordant and 72% with concordant results had complete biochemical success.
The use of two confirmatory tests in patients with PA results in discordant results in approximately 23% of cases. Patients having discordant confirmatory test results had a comparable rate of lateralized PA and underwent adrenalectomy with similar long-term outcome.
原发性醛固酮增多症(PA)是内分泌性高血压最常见的形式。根据内分泌学会实践指南,PA的诊断需要病理筛查试验结果以及确诊试验期间醛固酮水平不可被抑制。使用一种以上确诊试验进行序贯检测可能会导致试验结果不一致。
我们在德国Conn登记处的111例连续患者中,研究了卡托普利激发试验(CCT)和生理盐水输注试验(SIT)结果不一致与通过肾上腺静脉采血(AVS)进行的患者亚型分类及结局之间的关联。一致性定义为两种试验时醛固酮水平均不可被抑制,而不一致性定义为试验结果相互矛盾。患有单侧疾病的患者接受了肾上腺切除术(ADX)。使用PASO标准评估生化和临床结局。
111例患者中有85例(77%)CCT和SIT结果一致。尽管一致性和不一致性试验患者的基线特征具有可比性,但后者在试验后醛固酮水平显著更低(CCT:170 vs. 114pg/ml;SIT:139 vs. 101pg/ml;p = 0.004)。在试验结果不一致的患者中35%(n = 9)以及试验结果一致的患者中46%(n = 39),AVS提示为单侧PA。48例患者中有36例进行了ADX。试验结果不一致的患者中有86%以及试验结果一致的患者中有72%获得了完全生化缓解。
在PA患者中使用两种确诊试验,约23%的病例会出现结果不一致。确诊试验结果不一致的患者单侧PA发生率相当,并且接受肾上腺切除术的长期结局相似。