Lee Jun Seok, Son Dong Wuk, Lee Su Hun, Ki Sung Soon, Lee Sang Weon, Song Geun Sung, Woo Joon Bum, Kim Young Ha
Department of Neurosurgery, Pusan National University Yangsan Hospital, Yangsan, Korea.
Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Hospital, Yangsan, Korea.
J Korean Neurosurg Soc. 2022 Jan;65(1):96-106. doi: 10.3340/jkns.2021.0131. Epub 2021 Dec 29.
The most common complication of anterior cervical discectomy and fusion (ACDF) is cage subsidence and maintenance of disc height affects postoperative clinical outcomes. We considered cage subsidence as an inappropriate indicator for evaluating preservation of disc height. Thus, this study aimed to consider patients with complications such as reduced total disc height compared to that before surgery and evaluate the relevance of several factors before ACDF.
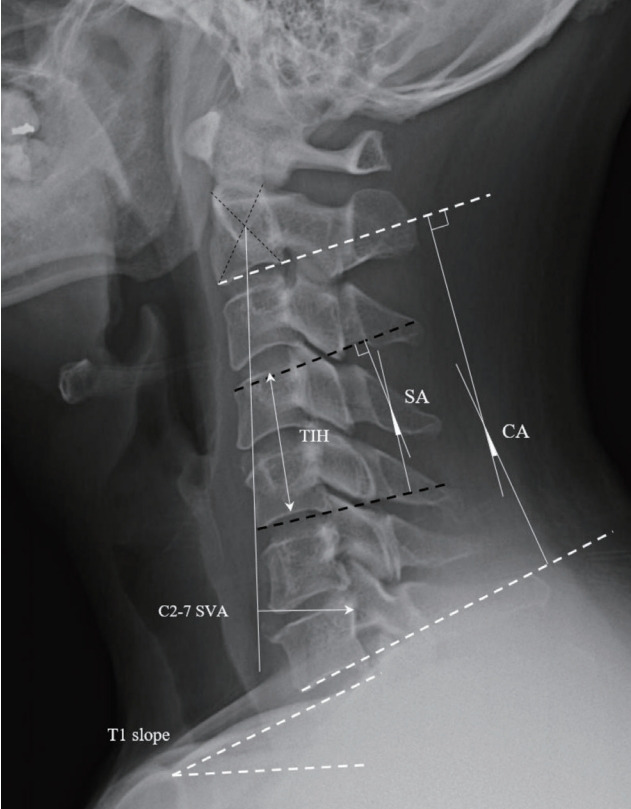
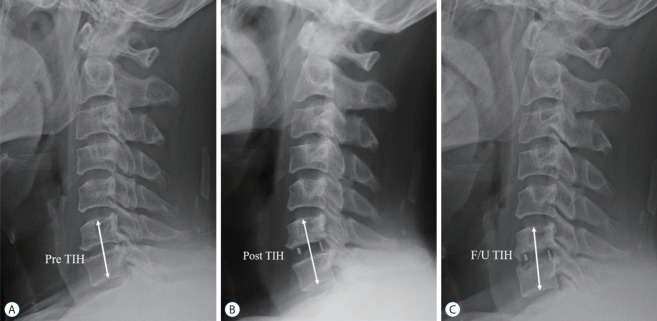
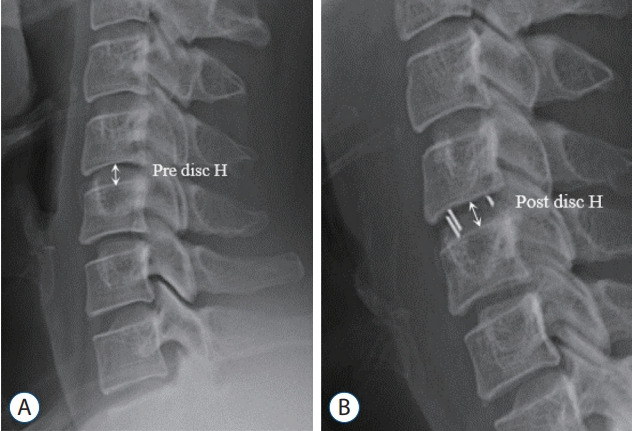
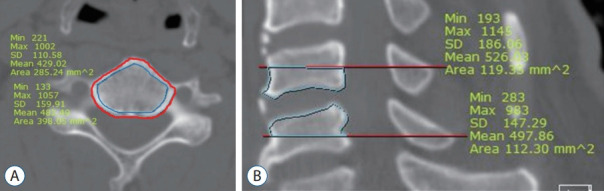
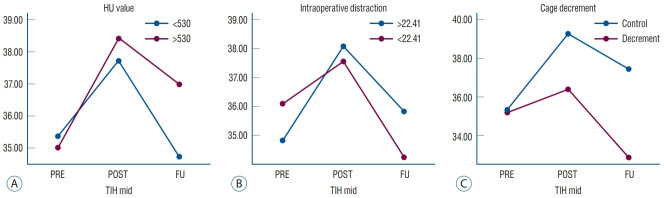
We retrospectively reviewed the medical records of 40 patients who underwent stand-alone single-level ACDF using a polyetheretherketone (PEEK) cage at our institution between January 2012 and December 2018. Our study population comprised 19 male and 21 female patients aged 24-70 years. The minimum follow-up period was 1 year. Twenty-seven patients had preoperative bone mineral density (BMD) data on dual-energy X-ray absorptiometry. Clinical parameters included sex, age, body mass index, smoking history, and prior medical history. Radiologic parameters included the C2-7 cobb angle, segmental angle, sagittal vertical axis, disc height, and total intervertebral height (TIH) at the preoperative and postoperative periods. Cage decrement was defined as the reduction in TIH at the 6-month follow-up compared to preoperative TIH. To evaluate the bone quality, Hounsfield unit (HU) value was calculated in the axial and sagittal images of conventional computed tomography.
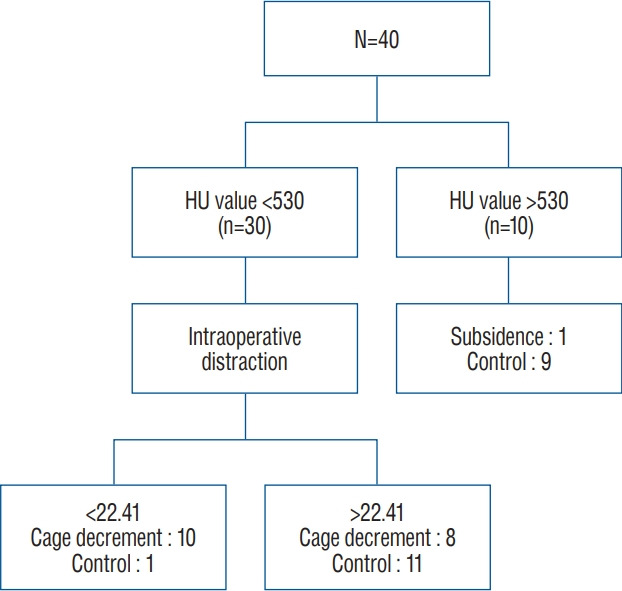
Lumbar BMD values and cervical HU values were significantly correlated (r=0.733, p<0.001). We divided the patients into two groups based on cage decrement, and 47.5% of the total patients were regarded as cage decrement. There were statistically significant differences in the parameters of measuring the HU value of the vertebra and intraoperative distraction between the two groups. Using these identified factors, we performed a receiver operating characteristic (ROC) curve analysis. Based on the ROC curve, the cut-off point was 530 at the HU value of the upper cortical and cancellous vertebrae (p=0.014; area under the curve [AUC], 0.727; sensitivity, 94.7%; specificity, 42.9%) and 22.41 at intraoperative distraction (p=0.017; AUC, 0.722; sensitivity, 85.7%; specificity, 57.9%). Using this value, we converted these parameters into a bifurcated variable and assessed the multinomial regression analysis to evaluate the risk factors for cage decrement in ACDF. Intraoperative distraction and HU value of the upper vertebral body were independent factors of postoperative subsidence.
Insufficient intraoperative distraction and low HU value showed a strong relationship with postoperative intervertebral height reduction following single stand-alone PEEK cage ACDF.
颈椎前路椎间盘切除融合术(ACDF)最常见的并发症是椎间融合器下沉,而维持椎间盘高度会影响术后临床疗效。我们认为椎间融合器下沉并非评估椎间盘高度保留情况的合适指标。因此,本研究旨在考量术前术后椎间盘总高度降低等并发症患者,并评估ACDF术前若干因素的相关性。
我们回顾性分析了2012年1月至2018年12月在我院接受聚醚醚酮(PEEK)椎间融合器单节段独立ACDF手术的40例患者的病历。研究对象包括19例男性和21例女性患者,年龄在24至70岁之间。最短随访期为1年。27例患者有双能X线吸收法测量的术前骨密度(BMD)数据。临床参数包括性别、年龄、体重指数、吸烟史和既往病史。影像学参数包括术前和术后的C2-7 Cobb角、节段角、矢状垂直轴、椎间盘高度和椎间总高度(TIH)。椎间融合器减量定义为6个月随访时TIH较术前TIH的降低值。为评估骨质,在传统计算机断层扫描的轴向和矢状图像上计算Hounsfield单位(HU)值。
腰椎BMD值与颈椎HU值显著相关(r = 0.733,p < 0.001)。我们根据椎间融合器减量将患者分为两组,47.5%的患者被视为有椎间融合器减量。两组在测量椎体HU值的参数和术中撑开方面存在统计学显著差异。利用这些确定的因素,我们进行了受试者工作特征(ROC)曲线分析。根据ROC曲线,上位皮质骨和松质骨HU值的截断点为530(p = 0.(此处原文有误,推测应为0.014);曲线下面积[AUC],0.72(此处原文有误,推测应为0.727);敏感性,94.7%;特异性,42.9%),术中撑开的截断点为22.41(p = 0.017;AUC,0.722;敏感性,85.7%;特异性,57.9%)。利用该值,我们将这些参数转换为二分变量,并进行多项回归分析以评估ACDF中椎间融合器减量的危险因素。术中撑开和上位椎体的HU值是术后下沉的独立因素。
术中撑开不足和低HU值与单节段独立PEEK椎间融合器ACDF术后椎间高度降低密切相关。