Depatment of Orthopaedic Surgery, Seoul National University College of Medicine, Seoul, Korea.
Clin Orthop Surg. 2011 Mar;3(1):16-23. doi: 10.4055/cios.2011.3.1.16. Epub 2011 Feb 15.
The purposes of the present study are to evaluate the subsidence and nonunion that occurred after anterior cervical discectomy and fusion using a stand-alone intervertebral cage and to analyze the risk factors for the complications.
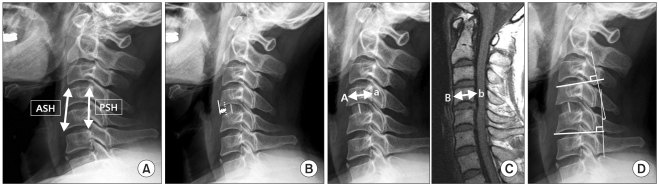
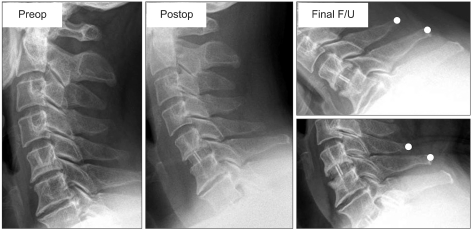
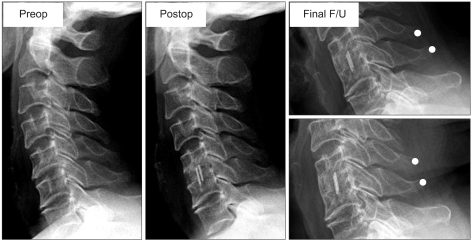
Thirty-eight patients (47 segments) who underwent anterior cervical fusion using a stand-alone polyetheretherketone (PEEK) cage and an autologous cancellous iliac bone graft from June 2003 to August 2008 were enrolled in this study. The anterior and posterior segmental heights and the distance from the anterior edge of the upper vertebra to the anterior margin of the cage were measured on the plain radiographs. Subsidence was defined as ≥ a 2 mm (minor) or 3 mm (major) decrease of the segmental height at the final follow-up compared to that measured at the immediate postoperative period. Nonunion was evaluated according to the instability being ≥ 2 mm in the interspinous distance on the flexion-extension lateral radiographs.
The anterior and posterior segmental heights decreased from the immediate postoperative period to the final follow-up at 1.33 ± 1.46 mm and 0.81 ± 1.27 mm, respectively. Subsidence ≥ 2 mm and 3 mm were observed in 12 segments (25.5%) and 7 segments (14.9%), respectively. Among the expected risk factors for subsidence, a smaller anteroposterior (AP) diameter (14 mm vs. 12 mm) of cages (p = 0.034; odds ratio [OR], 0.017) and larger intraoperative distraction (p = 0.041; OR, 3.988) had a significantly higher risk of subsidence. Intervertebral nonunion was observed in 7 segments (7/47, 14.9%). Compared with the union group, the nonunion group had a significantly higher ratio of two-level fusion to one-level fusions (p = 0.001).
Anterior cervical fusion using a stand-alone cage with a large AP diameter while preventing anterior intraoperative over-distraction will be helpful to prevent the subsidence of cages. Two-level cervical fusion might require more careful attention for avoiding nonunion.
本研究旨在评估使用独立椎间融合器行前路颈椎间盘切除融合术后的下沉和不愈合情况,并分析并发症的危险因素。
2003 年 6 月至 2008 年 8 月,38 例(47 个节段)患者接受前路融合术,使用聚醚醚酮(PEEK)独立椎间融合器和自体松质髂骨移植。在标准 X 线片上测量前路和后路节段高度以及上位椎体前缘至融合器前缘的距离。下沉定义为与术后即刻相比,终末随访时节段高度下降≥2mm(轻度)或 3mm(重度)。根据屈伸侧位 X 线片上的棘突间距离不稳定≥2mm 评估非融合。
术后即刻至终末随访时,前路和后路节段高度分别下降 1.33±1.46mm 和 0.81±1.27mm。12 个节段(25.5%)和 7 个节段(14.9%)出现下沉≥2mm 和 3mm。在下沉的预期危险因素中,融合器的前后径(14mm 比 12mm)较小(p=0.034;优势比[OR],0.017)和术中牵开较大(p=0.041;OR,3.988)与下沉风险显著增加相关。7 个节段(7/47,14.9%)发生椎间非融合。与融合组相比,非融合组 2 个节段融合与 1 个节段融合的比例显著更高(p=0.001)。
使用前后径较大的独立椎间融合器,同时防止术中前方过度牵开,有助于防止融合器下沉。对于 2 个节段的颈椎融合,需要更加小心,以避免非融合。