Department of Military and Community Medicine, Phramongkutklao College of Medicine, Bangkok 10400, Thailand.
Division of Nephrology and Hypertension, Mayo Clinic, Rochester, MN 55905, United States.
World J Gastroenterol. 2021 Dec 7;27(45):7831-7843. doi: 10.3748/wjg.v27.i45.7831.
Hepatorenal syndrome (HRS) is a life-threatening condition among patients with advanced liver disease. Data trends specific to hospital mortality and hospital admission resource utilization for HRS remain limited.
To assess the temporal trend in mortality and identify the predictors for mortality among hospital admissions for HRS in the United States.
We used the National Inpatient Sample database to identify an unweighted sample of 4938 hospital admissions for HRS from 2005 to 2014 (weighted sample of 23973 admissions). The primary outcomes were temporal trends in mortality as well as predictors for hospital mortality. We estimated odds ratios from multi-level mixed effect logistic regression to identify patient characteristics and treatments associated with hospital mortality.
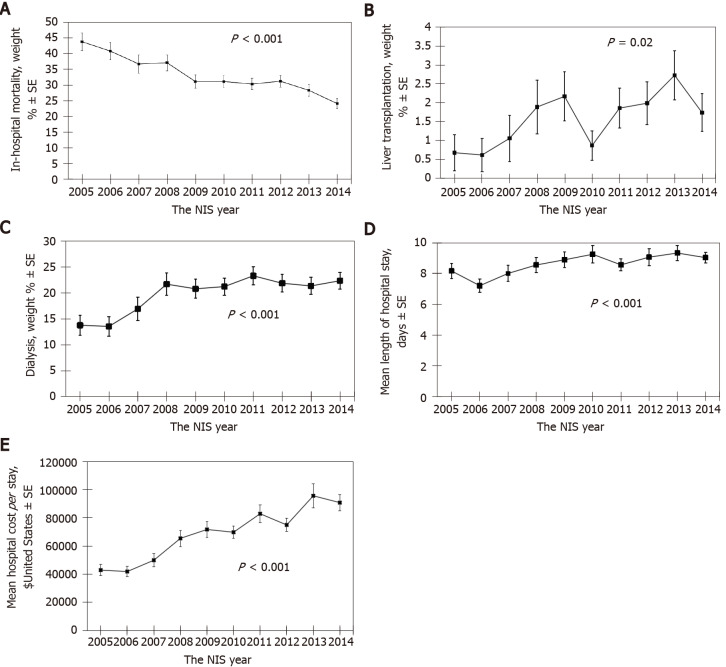
Overall hospital mortality was 32%. Hospital mortality decreased from 44% in 2005 to 24% in 2014 ( < 0.001), while there was an increase in the rate of liver transplantation ( = 0.02), renal replacement therapy ( < 0.001), length of hospital stay ( < 0.001), and hospitalization cost ( < 0.001). On multivariable analysis, older age, alcohol use, coagulopathy, neurological disorder, and need for mechanical ventilation predicted higher hospital mortality, whereas liver transplantation, transjugular intrahepatic portosystemic shunt, and abdominal paracentesis were associated with lower hospital mortality.
Although there was an increase in resource utilizations, hospital mortality among patients admitted for HRS significantly improved. Several predictors for hospital mortality were identified.
肝肾综合征(HRS)是一种危及生命的疾病,在晚期肝病患者中。关于 HRS 患者住院死亡率和住院资源利用的趋势数据仍然有限。
评估死亡率的时间趋势,并确定美国 HRS 住院患者死亡的预测因素。
我们使用国家住院患者样本数据库,从 2005 年到 2014 年确定了 4938 例 HRS 住院患者(未加权样本,23973 例)。主要结果是死亡率的时间趋势以及住院死亡率的预测因素。我们使用多水平混合效应逻辑回归估计比值比,以确定与住院死亡率相关的患者特征和治疗方法。
总体住院死亡率为 32%。2005 年的住院死亡率为 44%,2014 年降至 24%(<0.001),而肝移植(=0.02)、肾脏替代治疗(<0.001)、住院时间(<0.001)和住院费用(<0.001)的比率有所增加。多变量分析显示,年龄较大、饮酒、凝血障碍、神经障碍和需要机械通气与更高的住院死亡率相关,而肝移植、经颈静脉肝内门体分流术和腹腔穿刺术与更低的住院死亡率相关。
尽管资源利用有所增加,但 HRS 住院患者的死亡率显著降低。确定了几个与住院死亡率相关的预测因素。