Health Economics Research Centre, Nuffield Department of Population Health Sciences, Richard Doll Building, Old Road Campus, University of Oxford, Oxford OX3 7LF, UK.
Nuffield Department of Population Health Sciences, Richard Doll Building, Old Road Campus, University of Oxford, Oxford OX3 7LF, UK.
Age Ageing. 2022 Jan 6;51(1). doi: 10.1093/ageing/afab220.
hospital level healthcare in the home guided by comprehensive geriatric assessment (CGA) might provide a less costly alternative to hospitalisation for older people.
to determine the cost-effectiveness of CGA admission avoidance hospital at home (HAH) compared with hospital admission.
DESIGN/INTERVENTION: a cost-effectiveness study alongside a randomised trial of CGA in an admission avoidance HAH setting, compared with admission to hospital.
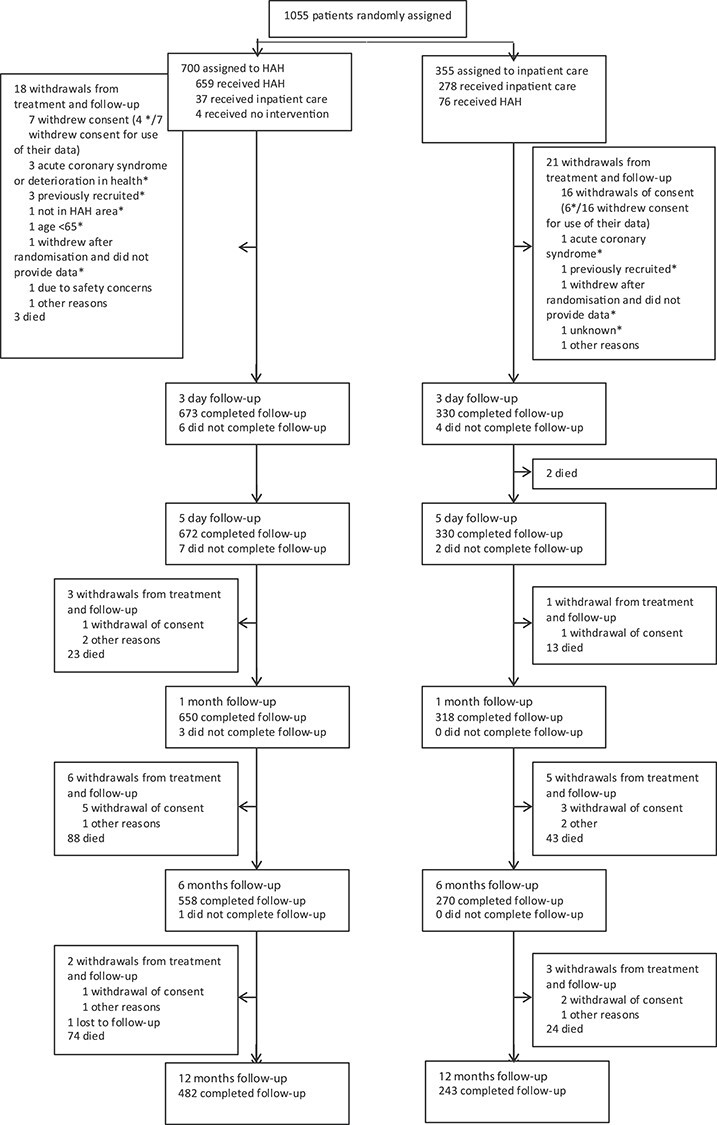
PARTICIPANTS/SETTING: older people considered for a hospital admission in nine locations across the UK were randomised using a 2:1 randomisation schedule to admission avoidance HAH with CGA (N = 700), or admission to hospital with CGA when available (N = 355).
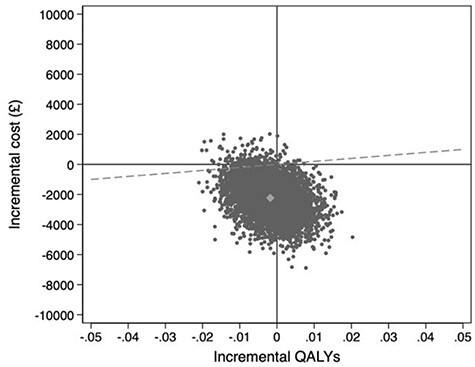
quality adjusted life years, resource use and costs at baseline and 6 months; incremental cost-effectiveness ratios were calculated. The main analysis used complete cases.
adjusting for baseline covariates, HAH was less costly than admission to hospital from a health and social care perspective (mean -£2,265, 95% CI: -4,279 to -252), and remained less costly with the addition of informal care costs (mean difference -£2,840, 95% CI: -5,495 to -185). There was no difference in quality adjusted survival. Using multiple imputation for missing data, the mean difference in health and social care costs widened to -£2,458 (95% CI: -4,977 to 61) and societal costs remained significantly lower (-£3,083, 95% CI: -5,880 to -287). There was little change to quality adjusted survival.
CGA HAH is a cost-effective alternative to admission to hospital for selected older people.
家庭综合老年评估(CGA)指导下的医院水平医疗保健可能为老年人提供比住院治疗成本更低的选择。
确定 CGA 入院避免家庭医院(HAH)与入院相比的成本效益。
设计/干预:在 CGA 入院避免 HAH 环境中进行随机试验的同时进行成本效益研究,与入院相比。
参与者/设置:在英国九个地点考虑住院的老年人,使用 2:1 的随机时间表,随机分配到 CGA 避免入院的 HAH(N=700)或在 CGA 可用时入院(N=355)。
基线和 6 个月时的质量调整生命年、资源使用和成本;计算增量成本效益比。主要分析使用完整病例。
从健康和社会护理的角度来看,HAH 比入院成本更低(平均-£2265,95%CI:-4279 至-252),并且在加入非正式护理成本后仍然更具成本效益(平均差异-£2840,95%CI:-5495 至-185)。生存质量调整无差异。对于缺失数据使用多重插补,健康和社会护理成本的平均差异扩大到-£2458(95%CI:-4977 至 61),社会成本仍然显著降低(-£3083,95%CI:-5880 至-287)。生存质量调整几乎没有变化。
对于选定的老年人,CGA HAH 是入院的一种具有成本效益的替代方案。