Department of Neurological Surgery, University of California, San Francisco, 505 Parnassus Ave., Rm. M-779, San Francisco, CA, 94143-0112, USA.
School of Medicine, University of California, San Francisco, San Francisco, CA, USA.
Acta Neurochir (Wien). 2022 Feb;164(2):405-417. doi: 10.1007/s00701-021-05067-9. Epub 2021 Dec 30.
There is a concern that glioma patients undergoing repeat craniotomies are more prone to complications. The study's goal was to assess if the complication profiles for initial and repeat craniotomies were similar, to determine predictors of complications, and to compare results with those in the literature.
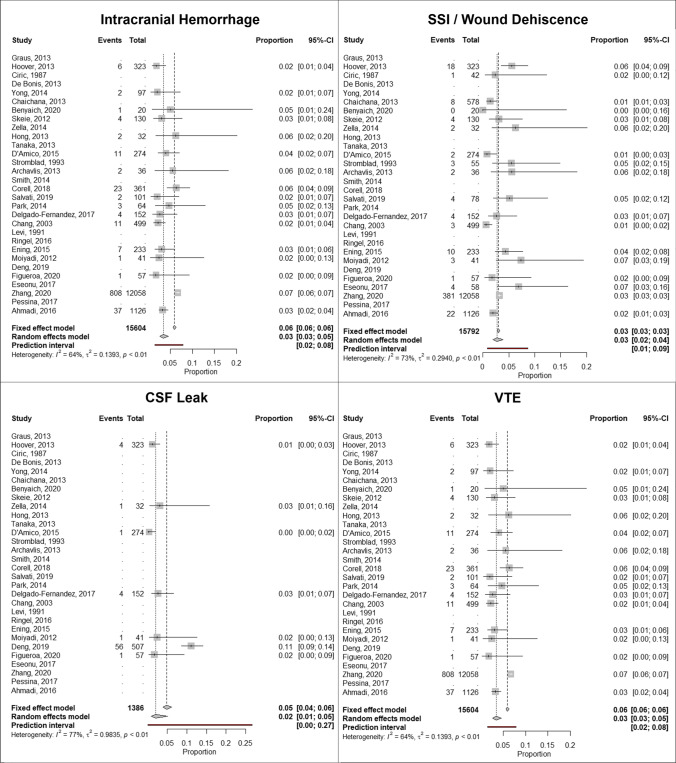
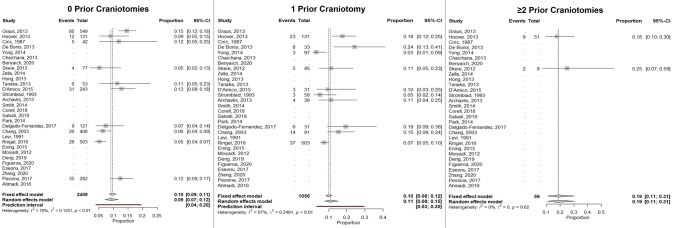
A retrospective study was conducted of glioma patients (WHO grade II-IV) who underwent either an initial or repeat craniotomy performed by the senior author from 2012 until 2019. Complications were recorded by discharge, 30 days, and 90 days postoperatively. New neurologic deficits were recorded by 90 days postoperatively. Multivariate regression was performed to identify factors associated with complications. A meta-analysis was performed to identify rates of complications based on number of prior craniotomies.
Within the cohort of 714 patients, 400 (56%) had no prior craniotomies, 218 (30.5%) had undergone 1 prior craniotomy, and 96 (13.5%) had undergone ≥ 2 prior craniotomies. There were 27 surgical and 10 medical complications in 30 patients (4.2%) and 19 reoperations for complications in 19 patients (2.7%) with no deaths by 90 days. Complications, reoperation rates, and new neurologic deficits did not differ based on number of prior craniotomies. On multivariate analysis, older age (OR1.5, 95%CI 1.0-2.2) and significant leukocytosis due to steroid use (OR12.6, 95%CI 2.5-62.9) were predictors of complications. Complication rates in the cohort were lower than rates reported in the literature.
Contrary to prior reports in the literature, repeat craniotomies can be as safe as initial operations if surgeons implement best practices.
有观点认为,接受再次开颅手术的脑胶质瘤患者更容易出现并发症。本研究旨在评估初次和再次开颅手术的并发症谱是否相似,确定并发症的预测因素,并与文献中的结果进行比较。
本研究回顾性分析了 2012 年至 2019 年由资深作者行初次或再次开颅手术的脑胶质瘤患者(世界卫生组织分级 II-IV 级)的临床资料。通过出院时、术后 30 天和 90 天记录并发症,术后 90 天记录新的神经功能缺损。采用多变量回归分析确定与并发症相关的因素。进行荟萃分析以确定基于既往开颅次数的并发症发生率。
在 714 例患者中,400 例(56%)无既往开颅手术史,218 例(30.5%)行 1 次既往开颅手术,96 例(13.5%)行≥2 次既往开颅手术。30 例患者(4.2%)发生 27 例手术并发症和 10 例医疗并发症,19 例患者(2.7%)因并发症行 19 次再次手术,90 天内无死亡病例。基于既往开颅次数,并发症、再次手术率和新的神经功能缺损无差异。多变量分析显示,年龄较大(OR1.5,95%CI 1.0-2.2)和因类固醇使用导致的显著白细胞增多(OR12.6,95%CI 2.5-62.9)是并发症的预测因素。本研究队列的并发症发生率低于文献报道的发生率。
如果外科医生实施最佳实践,再次开颅手术与初次手术一样安全,与文献中的先前报告相反。