Division of Cardiovascular Medicine, Loyola University Medical Center, Stritch School of Medicine, Maywood, IL, USA.
Department of Internal Medicine, Loyola University Medical Center, Maywood, IL, USA.
J Cardiovasc Magn Reson. 2022 Jan 3;24(1):3. doi: 10.1186/s12968-021-00831-3.
Atrial fibrillation (AF) is a progressive condition, which is characterized by inflammation/fibrosis of left atrial (LA) wall, an increase in the LA size/volumes, and decrease in LA function. We sought to investigate the relationship of anatomical and functional parameters obtained by cardiovascular magnetic resonance (CMR), with AF recurrence in paroxysmal AF (pAF) patients after catheter ablation.
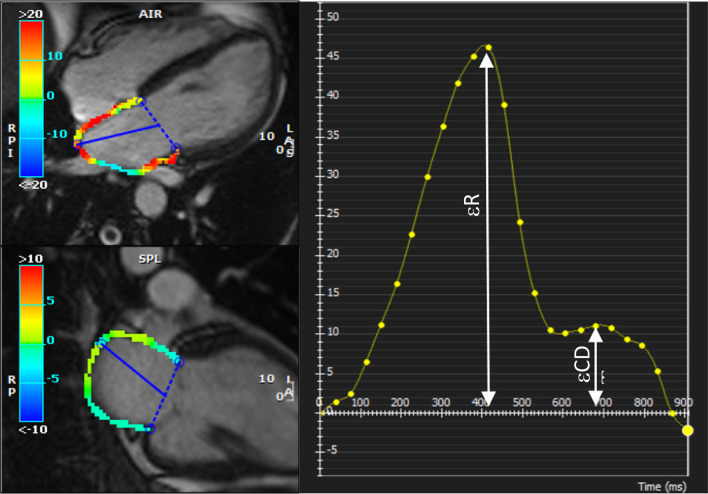
We studied 80 consecutive pAF patients referred for ablation, between January 2014 and December 2019, who underwent pre- and post-ablation CMR while in sinus rhythm. LA volumes were measured using the area-length method and included maximum, minimum, and pre-atrial-contraction volumes. CMR-derived LA reservoir strain (ℇR), conduit strain (ℇCD), and contractile strain (ℇCT) were measured by computer assisted manual planimetry. We used a multivariate logistical regression to estimate the independent predictors of AF recurrence after ablation.
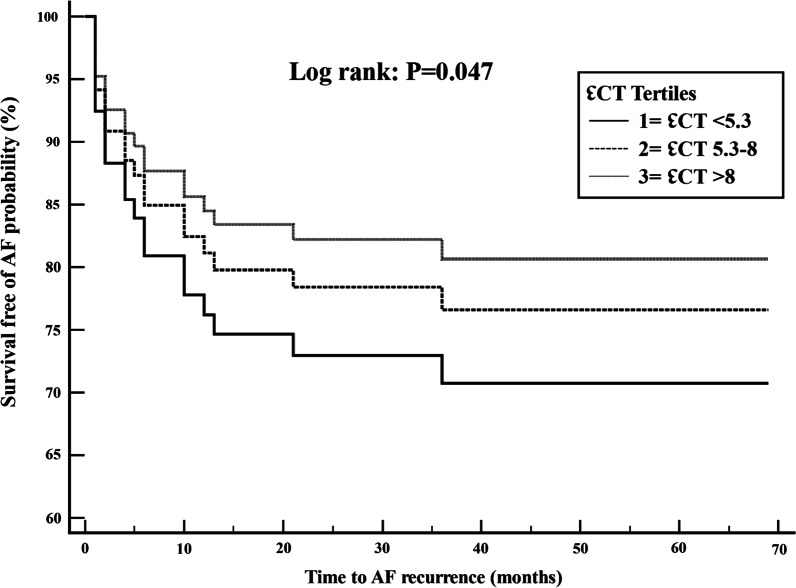
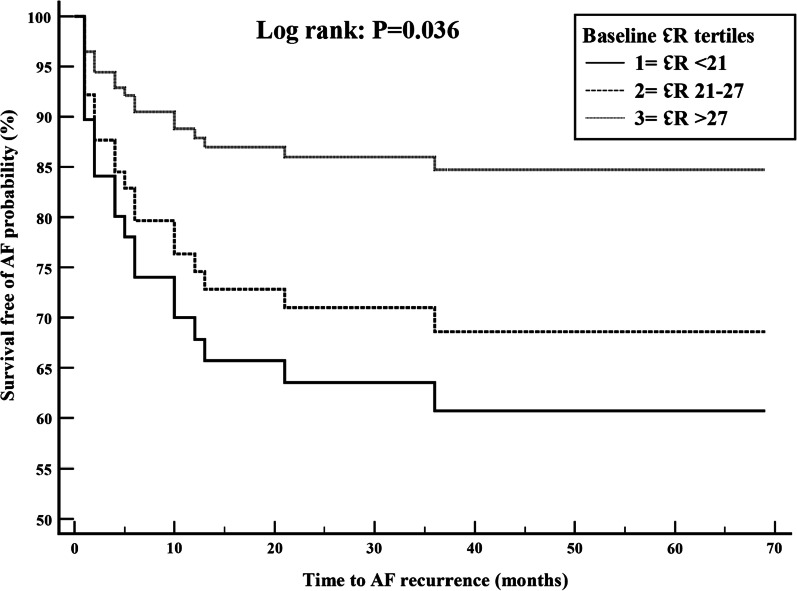
Mean age was 58.6 ± 9.4 years, 75% men, mean CHADS-VASc score was 1.7, 36% had prior cardioversion and 51% were taking antiarrhythmic drugs. Patients were followed for a median of 4 years (Q1-Q3 = 2.5-6.2 years). Of the 80 patients, 21 (26.3%) patients had AF recurrence after ablation. There were no significant differences between AF recurrence vs. no recurrence groups in age, gender, CHADS-VASc score, or baseline comorbidities. At baseline, patients with AF recurrence compared to without recurrence had lower LV end systolic volume index (32 ± 7 vs 37 ± 11 mL/m2; p = 0.045) and lower ℇCT (7.1 ± 4.6 vs 9.1 ± 3.7; p = 0.05). Post-ablation, patients with AF recurrence had higher LA minimum volume (68 ± 32 vs 55 ± 23; p = 0.05), right atrial volume index (62 ± 20 vs 52 ± 19 mL/m2; p = 0.04) and lower LA active ejection fraction (24 ± 8 vs 29 ± 11; p = 0.05), LA total ejection fraction (39 ± 14 vs 46 ± 12; p = 0.02), LA expansion index (73.6 ± 37.5 vs 94.7 ± 37.1; p = 0.03) and ℇCT (6.2 ± 2.9 vs 7.3 ± 1.7; p = 0.04). Adjusting for clinical variables in the multivariate logistic regression model, post-ablation minimum LA volume (OR 1.09; CI 1.02-1.16), LA expansion index (OR 0.98; CI 0.96-0.99), and baseline ℇR (OR 0.92; CI 0.85-0.99) were independently associated with AF recurrence.
Significant changes in LA volumes and strain parameters occur after AF ablation. CMR derived baseline ℇR, post-ablation minimum LAV, and expansion index are independently associated with AF recurrence.
心房颤动(AF)是一种进行性疾病,其特征在于左心房(LA)壁的炎症/纤维化、LA 大小/容积增加和 LA 功能下降。我们旨在研究通过心血管磁共振(CMR)获得的解剖学和功能参数与阵发性 AF(pAF)患者消融后 AF 复发之间的关系。
我们研究了 2014 年 1 月至 2019 年 12 月期间因消融而转诊的 80 例连续 pAF 患者,他们在窦性心律时接受了消融前和消融后的 CMR。使用面积-长度法测量 LA 容积,包括最大、最小和心房收缩前容积。通过计算机辅助手动平面测量法测量 CMR 衍生的 LA 储备应变(ℇR)、导联应变(ℇCD)和收缩应变(ℇCT)。我们使用多变量逻辑回归来估计消融后 AF 复发的独立预测因子。
平均年龄为 58.6±9.4 岁,75%为男性,平均 CHADS-VASc 评分为 1.7,36%曾接受过电复律,51%服用抗心律失常药物。患者的中位随访时间为 4 年(Q1-Q3=2.5-6.2 年)。在 80 例患者中,21 例(26.3%)患者在消融后出现 AF 复发。AF 复发组与无复发组在年龄、性别、CHADS-VASc 评分或基线合并症方面无显著差异。基线时,与无复发组相比,AF 复发组的左心室射血末期容积指数较低(32±7 vs 37±11 ml/m2;p=0.045),而 ℇCT 较低(7.1±4.6 vs 9.1±3.7;p=0.05)。消融后,AF 复发组的 LA 最小容积较高(68±32 vs 55±23;p=0.05),右心房容积指数较高(62±20 vs 52±19 ml/m2;p=0.04),LA 主动射血分数较低(24±8 vs 29±11;p=0.05),LA 总射血分数较低(39±14 vs 46±12;p=0.02),LA 扩张指数较高(73.6±37.5 vs 94.7±37.1;p=0.03),而 ℇCT 较低(6.2±2.9 vs 7.3±1.7;p=0.04)。在多变量逻辑回归模型中调整临床变量后,消融后最小 LA 容积(OR 1.09;95%CI 1.02-1.16)、LA 扩张指数(OR 0.98;95%CI 0.96-0.99)和基线 ℇR(OR 0.92;95%CI 0.85-0.99)与 AF 复发独立相关。
AF 消融后 LA 容积和应变参数发生显著变化。CMR 衍生的基线 ℇR、消融后最小 LA 容积和扩张指数与 AF 复发独立相关。