Szaro Pawel, McGrath Alexandra, Ciszek Bogdan, Geijer Mats
Department of Radiology, Institute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden.
Department of Musculoskeletal Radiology, Sahlgrenska University Hospital, Gothenburg, Sweden.
Eur J Radiol Open. 2021 Dec 20;9:100392. doi: 10.1016/j.ejro.2021.100392. eCollection 2022.
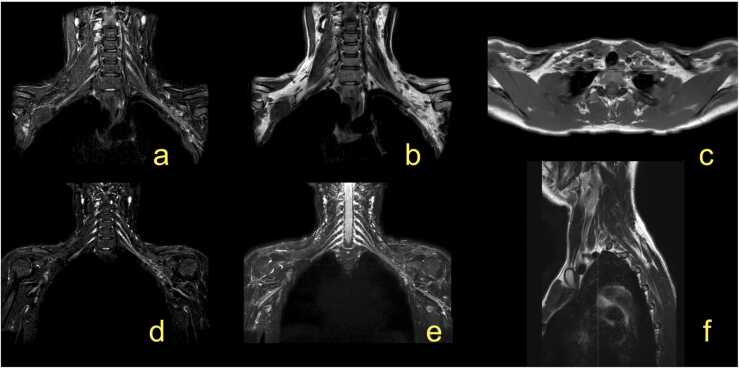
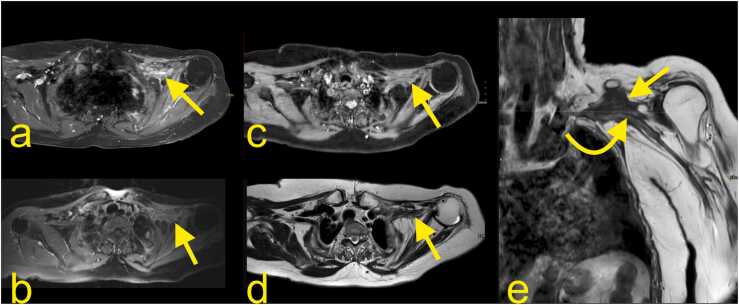
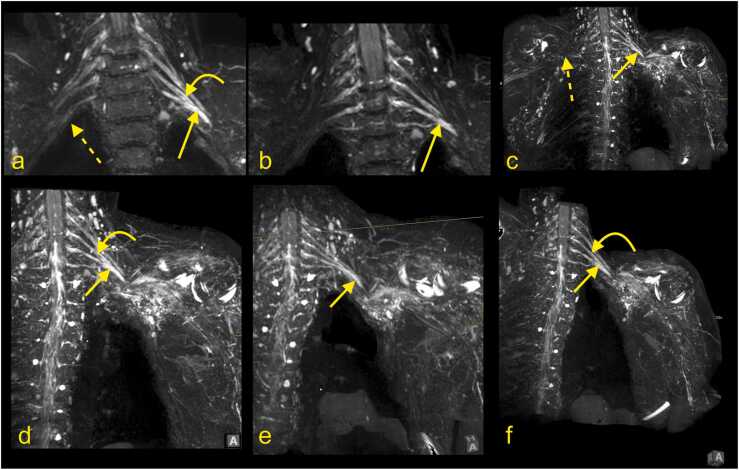
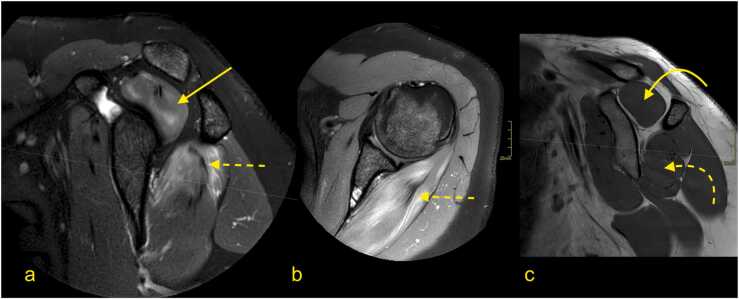
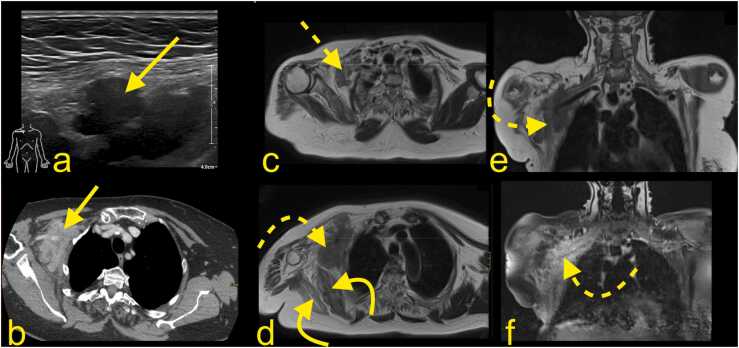
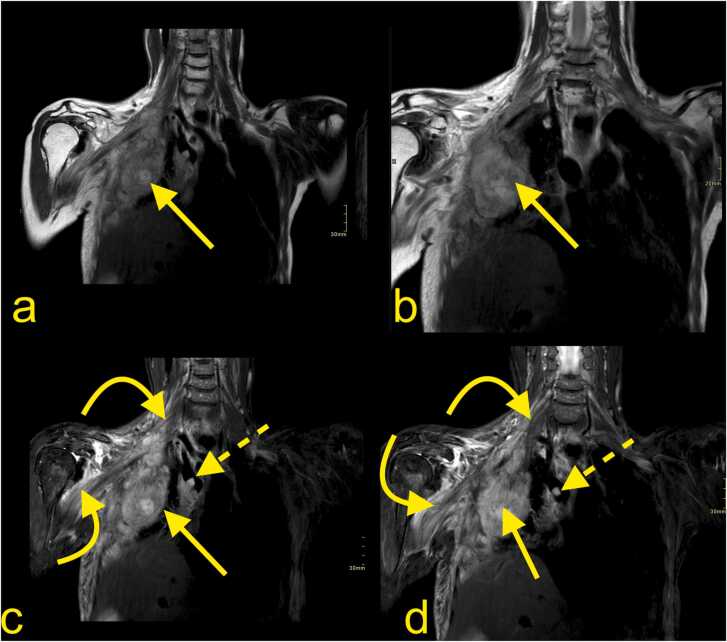
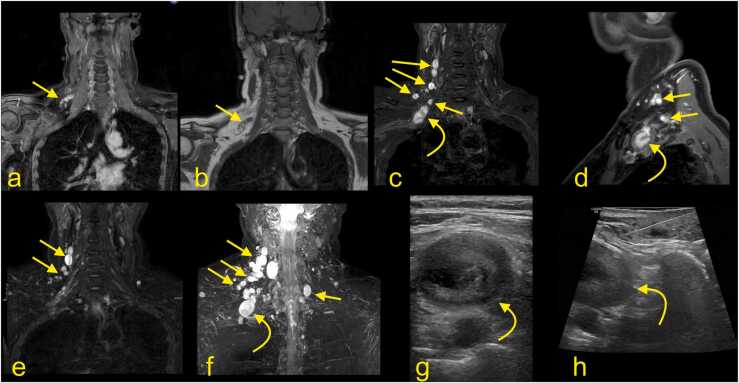
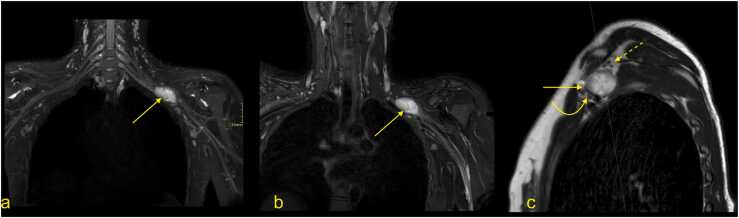
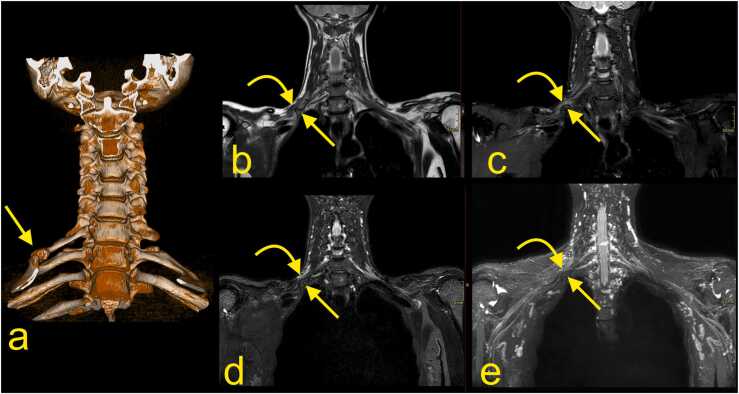
For magnetic resonance imaging (MRI) of non-traumatic brachial plexus (BP) lesions, sequences with contrast injection should be considered in the differentiation between tumors, infection, postoperative conditions, and post-radiation changes. The most common non-traumatic inflammatory BP neuropathy is radiation neuropathy. T2-weighted images may help to distinguish neoplastic infiltration showing a high signal from radiation-induced neuropathy with fibrosis presenting a low signal. MRI findings in inflammatory BP neuropathy are usually absent or discrete. Diffuse edema of the BP localized mainly in the supraclavicular part of BP, with side-to-side differences, and shoulder muscle denervation may be found on MRI. BP infection is caused by direct infiltration from septic arthritis of the shoulder joint, spondylodiscitis, or lung empyema. MRI may help to narrow down the list of differential diagnoses of tumors. The most common tumor of BP is metastasis. The most common primary tumor of BP is neurofibroma, which is visible as fusiform thickening of a nerve. In its solitary state, it may be challenging to differentiate from a schwannoma. The most common MRI finding is a neurogenic variant of thoracic outlet syndrome with an asymmetry of signal and thickness of the BP with edema. In abduction, a loss of fat directly related to the BP may be seen. Diffusion tensor imaging is a promising novel MRI sequences; however, the small diameter of the nerves contributing to the BP and susceptibility to artifacts may be challenging in obtaining sufficiently high-quality images.
对于非创伤性臂丛神经(BP)病变的磁共振成像(MRI),在鉴别肿瘤、感染、术后情况和放疗后改变时,应考虑使用注射对比剂的序列。最常见的非创伤性炎性BP神经病是放射性神经病。T2加权图像可能有助于区分显示高信号的肿瘤浸润与表现为低信号纤维化的放射性神经病。炎性BP神经病的MRI表现通常不明显或呈散在分布。BP的弥漫性水肿主要局限于BP的锁骨上部分,存在双侧差异,MRI上可能发现肩部肌肉失神经支配。BP感染由肩关节化脓性关节炎、脊椎椎间盘炎或肺脓肿直接蔓延所致。MRI有助于缩小肿瘤的鉴别诊断范围。BP最常见的肿瘤是转移瘤。BP最常见的原发性肿瘤是神经纤维瘤,表现为神经的梭形增粗。在孤立状态下,它可能难以与神经鞘瘤相鉴别。最常见的MRI表现是胸廓出口综合征的神经源性变异,BP的信号和厚度不对称并伴有水肿。在外展时,可能会看到与BP直接相关的脂肪缺失。扩散张量成像(DTI)是一种很有前景的新型MRI序列;然而,构成BP的神经直径较小且易受伪影影响,可能难以获得足够高质量的图像。