Department of Radiation Medicine and Applied Sciences, University of California San Diego, La Jolla, California, USA.
School of Public Health, Division of Health Management and Policy, San Diego State University, San Diego, California, USA.
Cancer Med. 2022 Feb;11(4):1192-1201. doi: 10.1002/cam4.4518. Epub 2022 Jan 5.
Oncology rapidly shifted to telemedicine in response to the COVID-19 pandemic. Telemedicine can increase access to healthcare, but recent research has shown disparities exist with telemedicine use during the pandemic. This study evaluated health disparities associated with telemedicine uptake during the COVID-19 pandemic among cancer patients in a tertiary care academic medical center.
This retrospective cohort study evaluated telemedicine use among adult cancer patients who received outpatient medical oncology care within a tertiary care academic healthcare system between January and September 2020. We used multivariable mixed-effects logistic regression models to determine how telemedicine use varied by patient race/ethnicity, primary language, insurance status, and income level. We assessed geospatial links between zip-code level COVID-19 infection rates and telemedicine use.
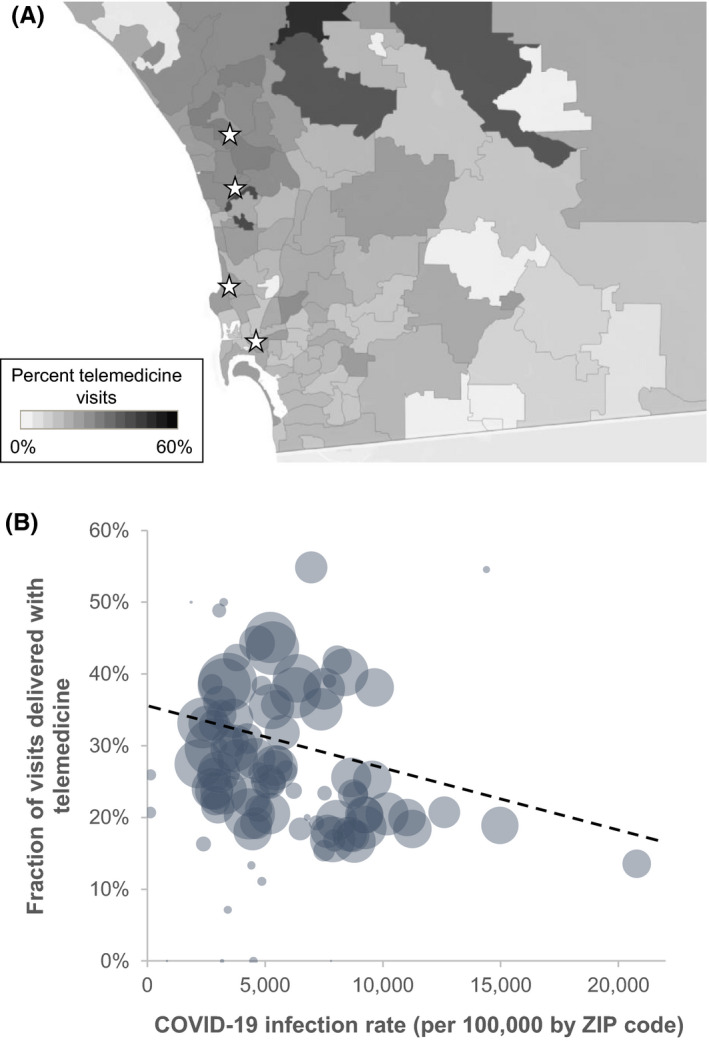
Among 29,421 patient encounters over the study period, 8,541 (29%) were delivered via telemedicine. Several groups of patients were less likely to use telemedicine, including Hispanic (adjusted odds ratio [aOR] 0.86, p = 0.03), Asian (aOR 0.79, p = 0.002), Spanish-speaking (aOR 0.71, p = 0.0006), low-income (aOR 0.67, p < 0.0001), and those with Medicaid (aOR 0.66, p < 0.0001). Lower rates of telemedicine use were found in zip codes with higher rates of COVID-19 infection. Each 10% increase in COVID-19 infection rates was associated with an 8.3% decrease in telemedicine use (p = 0.002).
This study demonstrates racial/ethnic, language, and income-level disparities with telemedicine use, which ultimately led patients with the highest risk of COVID-19 infection to use telemedicine the least. Additional research to better understand actionable barriers will help improve telemedicine access among our underserved populations.
由于 COVID-19 大流行,肿瘤学迅速转向远程医疗。远程医疗可以增加获得医疗保健的机会,但最近的研究表明,在大流行期间使用远程医疗存在差异。本研究评估了在一家三级保健学术医疗中心的癌症患者中,与 COVID-19 大流行期间远程医疗接受度相关的健康差异。
本回顾性队列研究评估了在 2020 年 1 月至 9 月期间,在一家三级保健学术医疗系统中接受门诊肿瘤学治疗的成年癌症患者中远程医疗的使用情况。我们使用多变量混合效应逻辑回归模型来确定远程医疗的使用情况如何因患者的种族/民族、主要语言、保险状况和收入水平而异。我们评估了邮政编码级别的 COVID-19 感染率与远程医疗使用之间的地理空间联系。
在研究期间的 29421 次患者就诊中,有 8541 次(29%)通过远程医疗提供。一些患者群体不太可能使用远程医疗,包括西班牙裔(调整后的优势比 [aOR] 0.86,p=0.03)、亚裔(aOR 0.79,p=0.002)、西班牙语裔(aOR 0.71,p=0.0006)、低收入(aOR 0.67,p<0.0001)和有医疗补助的人(aOR 0.66,p<0.0001)。在 COVID-19 感染率较高的邮政编码中,远程医疗的使用频率较低。COVID-19 感染率每增加 10%,远程医疗的使用就会减少 8.3%(p=0.002)。
本研究表明,在使用远程医疗方面存在种族/民族、语言和收入水平的差异,这最终导致感染 COVID-19 风险最高的患者使用远程医疗的频率最低。进一步研究以更好地了解可采取的障碍将有助于改善我们服务不足的人群的远程医疗机会。