Department of Cardiovascular Medicine, Gunma University Graduate School of Medicine, 3-39-22 Showa-machi, Maebashi, Gunma, 371-8511, Japan.
Division of Cardiovascular Medicine, National Defense Medical College, Tokorozawa, Saitama, Japan.
Sci Rep. 2022 Jan 7;12(1):13. doi: 10.1038/s41598-021-03974-6.
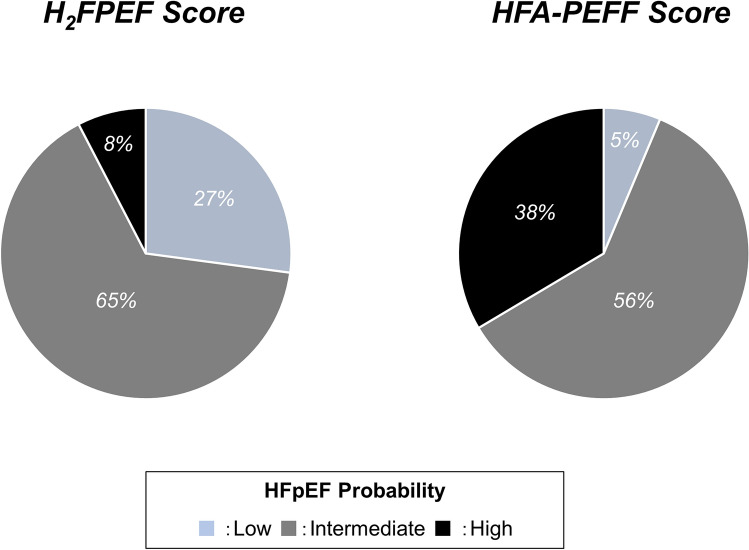
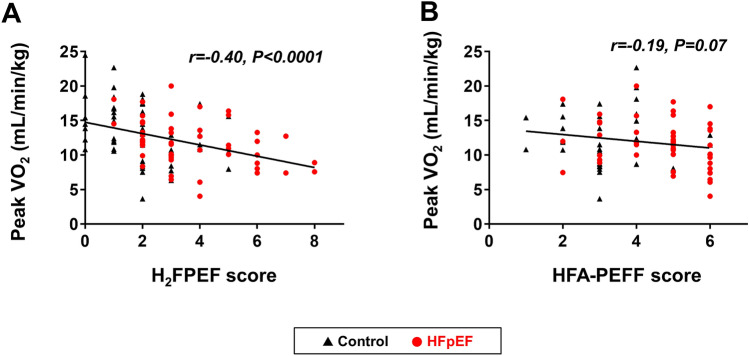
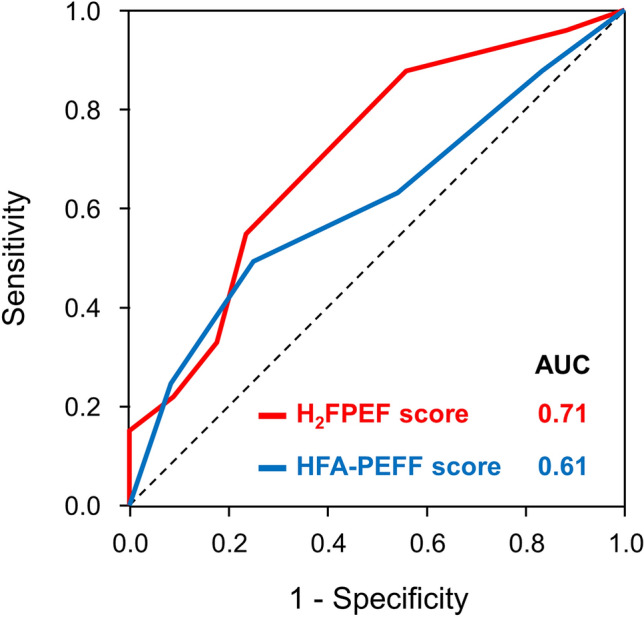
Exercise intolerance is a primary manifestation in patients with heart failure with preserved ejection fraction (HFpEF) and is associated with abnormal hemodynamics and a poor quality of life. Two multiparametric scoring systems have been proposed to diagnose HFpEF. This study sought to determine the performance of the HFPEF and HFA-PEFF scores for predicting exercise capacity and echocardiographic findings of intracardiac pressures during exercise in subjects with dyspnea on exertion referred for bicycle stress echocardiography. In a subset, simultaneous expired gas analysis was performed to measure the peak oxygen consumption (VO). Patients with HFpEF (n = 83) and controls without HF (n = 104) were enrolled. The HFPEF score was obtainable for all patients while the HFA-PEFF score could not be calculated for 23 patients (feasibility 88%). Both HFPEF and HFA-PEFF scores correlated with a higher E/e' ratio (r = 0.49 and r = 0.46), lower systolic tricuspid annular velocity (r = - 0.44 and = - 0.24), and lower cardiac output (r = - 0.28 and r = - 0.24) during peak exercise. Peak VO and exercise duration decreased with an increase in HFPEF scores (r = - 0.40 and r = - 0.32). The HFPEF score predicted a reduced aerobic capacity (AUC 0.71, p = 0.0005), but the HFA-PEFF score did not (p = 0.07). These data provide insights into the role of the HFPEF and HFA-PEFF scores for predicting exercise intolerance and abnormal hemodynamics in patients presenting with exertional dyspnea.
运动不耐受是射血分数保留心力衰竭(HFpEF)患者的主要表现,与异常血液动力学和较差的生活质量有关。已经提出了两种多参数评分系统来诊断 HFpEF。本研究旨在确定 HFPEF 和 HFA-PEFF 评分在预测运动能力和运动时心内压力的超声心动图表现方面的性能,这些患者因运动性呼吸困难而接受自行车运动超声心动图检查。在亚组中,同时进行呼出气体分析以测量峰值摄氧量(VO)。共纳入 83 例 HFpEF 患者和 104 例无 HF 对照者。所有患者均可获得 HFPEF 评分,而 23 例患者无法计算 HFA-PEFF 评分(可行性 88%)。HFPEF 和 HFA-PEFF 评分均与较高的 E/e' 比值相关(r=0.49 和 r=0.46),较低的收缩期三尖瓣环速度(r=-0.44 和 r=-0.24)和较低的心输出量(r=-0.28 和 r=-0.24)相关。峰值 VO 和运动持续时间随 HFPEF 评分的增加而降低(r=-0.40 和 r=-0.32)。HFPEF 评分预测有氧能力降低(AUC 0.71,p=0.0005),但 HFA-PEFF 评分则不然(p=0.07)。这些数据提供了 HFPEF 和 HFA-PEFF 评分在预测运动不耐受和运动性呼吸困难患者异常血液动力学方面的作用的见解。