Department of General Surgery, Changzhou Hospital of Traditional Chinese Medicine, Changzhou, China.
Department of Pediatric Cardiology, Xinhua Hospital, Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, China.
Front Immunol. 2021 Dec 23;12:769685. doi: 10.3389/fimmu.2021.769685. eCollection 2021.
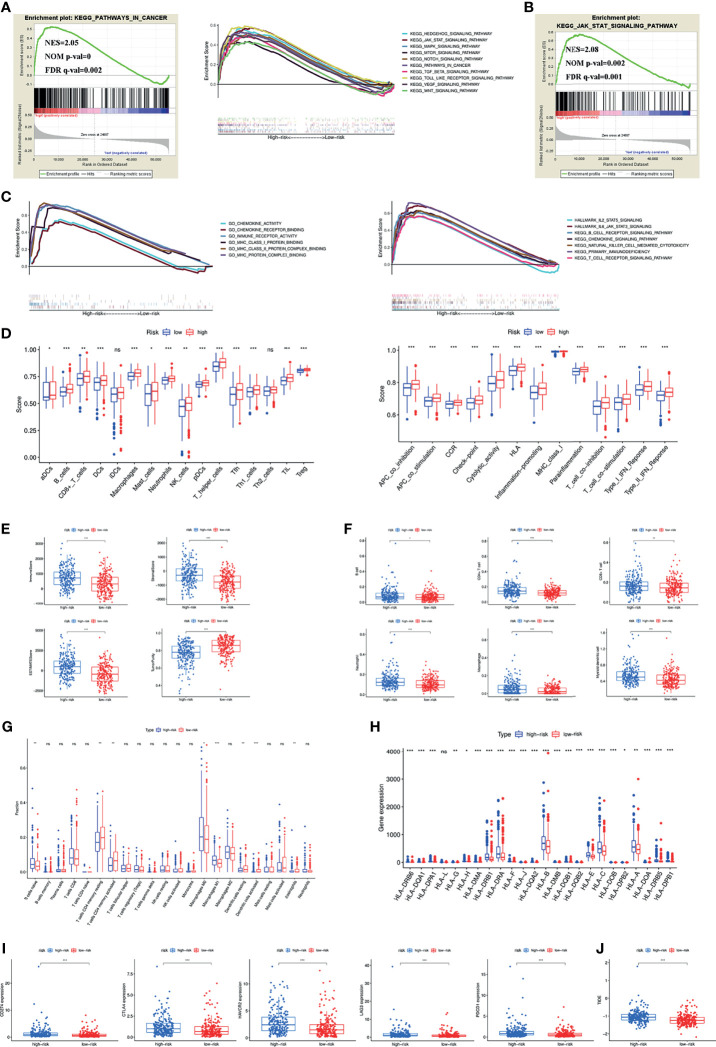
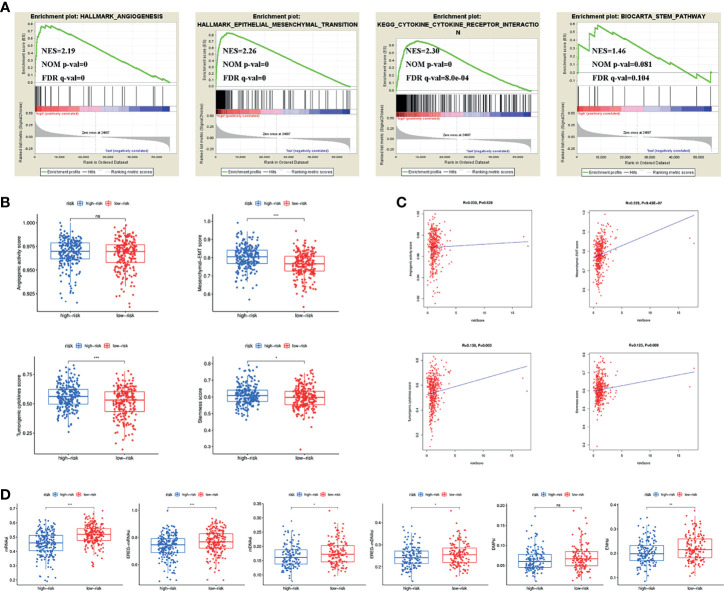
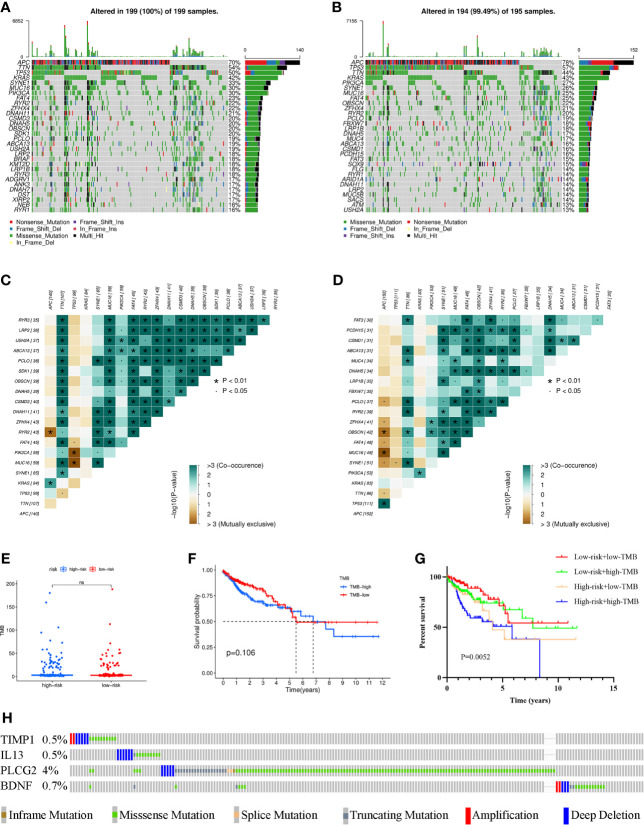
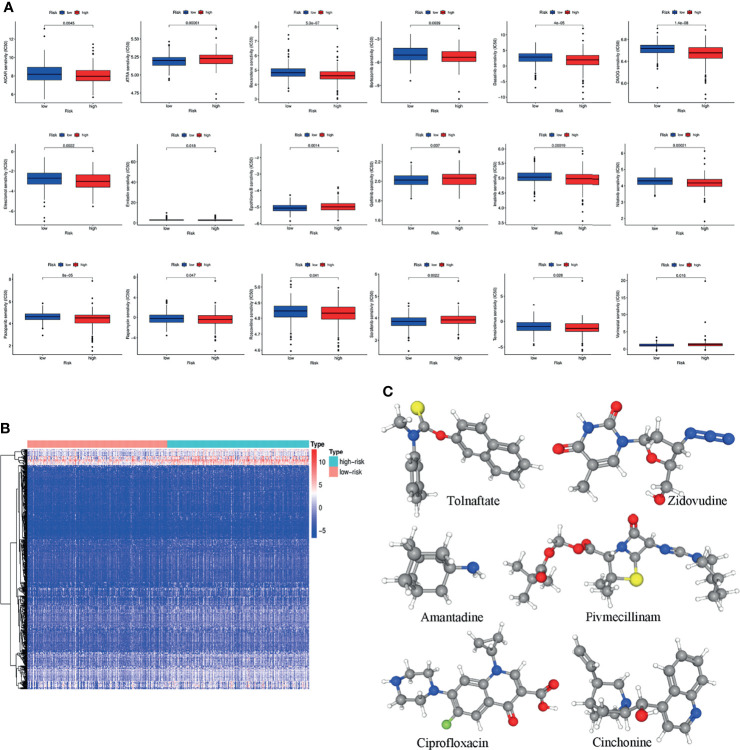
Both tumour-infiltrating immune cells and inflammation-related genes that can mediate immune infiltration contribute to the initiation and prognosis of patients with colon cancer. In this study, we developed a method to predict the survival outcomes among colon cancer patients and direct immunotherapy and chemotherapy. We obtained patient data from The Cancer Genome Atlas (TCGA) and captured inflammation-related genes from the GeneCards database. The package "ConsensusClusterPlus" was used to generate molecular subtypes based on inflammation-related genes obtained by differential expression analysis and univariate Cox analysis. A prognostic signature including four genes (PLCG2, TIMP1, BDNF and IL13) was also constructed and was an independent prognostic factor. Cluster 2 and higher risk scores meant worse overall survival and higher expression of human leukocyte antigen and immune checkpoints. Immune cell infiltration calculated by the estimate, CIBERSORT, TIMER, ssGSEA algorithms, tumour immune dysfunction and exclusion (TIDE), and tumour stemness indices (TSIs) were also compared on the basis of inflammation-related molecular subtypes and the risk signature. In addition, analyses of stratification, somatic mutation, nomogram construction, chemotherapeutic response prediction and small-molecule drug prediction were performed based on the risk signature. We finally used qRT-PCR to detect the expression levels of four genes in colon cancer cell lines and obtained results consistent with the prediction. Our findings demonstrated a four-gene prognostic signature that could be useful for prognostication in colon cancer patients and designing personalized treatments, which could provide new versions of personalized management for these patients.
肿瘤浸润免疫细胞和炎症相关基因均可介导免疫浸润,从而促进结直肠癌的发生和发展。在本研究中,我们开发了一种方法,用于预测结直肠癌患者的生存结局,并指导免疫治疗和化疗。我们从癌症基因组图谱(TCGA)获取患者数据,并从基因卡片数据库获取炎症相关基因。使用“ConsensusClusterPlus”软件包基于差异表达分析和单变量 Cox 分析获得的炎症相关基因生成分子亚型。还构建了一个包含四个基因(PLCG2、TIMP1、BDNF 和 IL13)的预后特征,并证实其是一个独立的预后因素。聚类 2 和更高的风险评分意味着更差的总生存率和更高的人类白细胞抗原和免疫检查点表达。还基于炎症相关的分子亚型和风险特征,比较了估计、CIBERSORT、TIMER、ssGSEA 算法、肿瘤免疫功能障碍和排除(TIDE)和肿瘤干性指数(TSIs)计算的免疫细胞浸润。此外,还基于风险特征进行了分层分析、体细胞突变分析、列线图构建、化疗反应预测和小分子药物预测分析。最后,我们使用 qRT-PCR 检测了结直肠癌细胞系中四个基因的表达水平,结果与预测一致。我们的研究结果表明,一个四基因预后特征可用于预测结直肠癌患者的预后和设计个性化治疗方案,为这些患者提供新的个性化管理方案。