Wang Qian, Xiao Xinguang, Liang Yanchang, Wen Hao, Wen Xiaopeng, Gu Meilan, Ren Cuiping, Li Kunbin, Yu Liangwen, Lu Liming
Department of Medical Imaging, Zhengzhou Central Hospital Affiliated to Zhengzhou University, 195 Tongbai Road, 455007, Zhengzhou, China.
Guangzhou University of Chinese Medicine, 510006, Guangzhou, China.
J Cancer. 2021 Oct 28;12(24):7399-7412. doi: 10.7150/jca.62131. eCollection 2021.
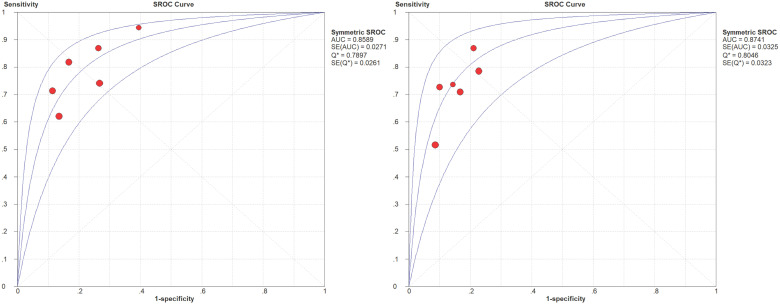
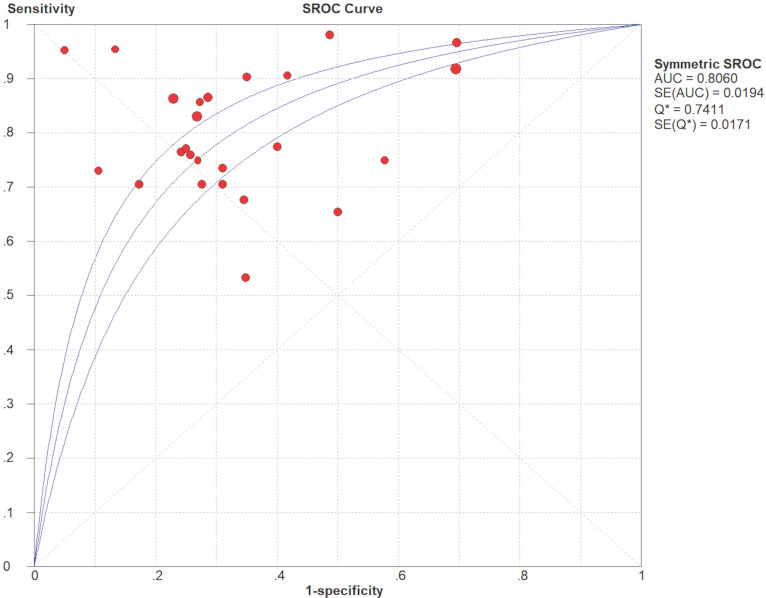
To evaluate the diagnostic performance of standard diffusion-weighted imaging (DWI), intravoxel incoherent motion (IVIM), and diffusion kurtosis imaging (DKI), for differentiating benign and malignant soft tissue tumors (STTs). A thorough search was carried out to identify suitable studies published up to September 2020. The quality of the studies involved was evaluated using Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2). The pooled sensitivity (SEN), specificity (SPE), and summary receiver operating characteristic (SROC) curve were calculated using bivariate mixed effects models. A subgroup analysis was also performed to explore the heterogeneity. Eighteen studies investigating 1319 patients with musculoskeletal STTs (malignant, =623; benign, =696) were enrolled. Thirteen standard DWI studies using the apparent diffusion coefficient (ADC) showed that the pooled SEN and SPE of ADC were 0.80 (95% CI: 0.77-0.82) and 0.63 (95% CI: 0.60-0.67), respectively. The area under the curve (AUC) calculated from the SROC curve was 0.806. The subgroup analysis indicated that the percentage of myxoid malignant tumors, magnet strength, study design, and ROI placement were significant factors affecting heterogeneity. Four IVIM studies showed that the AUCs calculated from the SROC curves of the parameters ADC and D were 0.859 and 0.874, respectively. The AUCs for the IVIM parameters pseudo diffusion coefficient (D*) and perfusion fraction (f) calculated from the SROC curve were 0.736 and 0.573, respectively. Two DKI studies showed that the AUCs of the DKI parameter mean kurtosis (MK) were 0.97 and 0.89, respectively. The DWI-derived ADC value and the IVIM DWI-derived D value might be accurate tools for discriminating musculoskeletal STTs, especially for non-myxoid SSTs, using more than two b values, with maximal b value ranging from 600 to 800 s/mm, additionally, a high-field strength (3.0 T) optimizes the diagnostic performance.
为评估标准扩散加权成像(DWI)、体素内不相干运动(IVIM)和扩散峰度成像(DKI)在鉴别良性和恶性软组织肿瘤(STT)方面的诊断性能。进行了全面检索以识别截至2020年9月发表的合适研究。使用诊断准确性研究质量评估-2(QUADAS-2)对所涉研究的质量进行评估。使用双变量混合效应模型计算合并敏感度(SEN)、特异度(SPE)和汇总接收器操作特征(SROC)曲线。还进行了亚组分析以探讨异质性。纳入了18项研究,共1319例肌肉骨骼STT患者(恶性,=623例;良性,=696例)。13项使用表观扩散系数(ADC)的标准DWI研究表明,ADC的合并SEN和SPE分别为0.80(95%CI:0.77-0.82)和0.63(95%CI:0.60-0.67)。从SROC曲线计算的曲线下面积(AUC)为0.806。亚组分析表明,黏液样恶性肿瘤的百分比、磁体强度、研究设计和感兴趣区(ROI)放置是影响异质性的显著因素。4项IVIM研究表明,参数ADC和D的SROC曲线计算的AUC分别为0.859和0.874。从SROC曲线计算的IVIM参数伪扩散系数(D*)和灌注分数(f)的AUC分别为0.736和0.573。2项DKI研究表明,DKI参数平均峰度(MK)的AUC分别为0.97和0.89。DWI衍生的ADC值和IVIM DWI衍生的D值可能是鉴别肌肉骨骼STT的准确工具,尤其是对于非黏液样SST,使用两个以上的b值,最大b值范围为600至800 s/mm,此外,高场强(3.0 T)可优化诊断性能。