Children's Neurosciences, Evelina London Children's Hospital, Guy's and St Thomas' NHS Foundation Trust, London, United Kingdom.
Queen Square MS Centre, UCL Queen Square Institute of Neurology, Faculty of Brain Sciences, University College London, London, United Kingdom.
Ann Clin Transl Neurol. 2022 Jan;9(1):67-78. doi: 10.1002/acn3.51494. Epub 2022 Jan 11.
To describe the clinical presentation, investigations, management, and disease course in pediatric autoimmune limbic encephalitis (LE).
In this retrospective observational study, from the UK Childhood Neuroinflammatory Disease network, we identified children from six tertiary centers with LE <18 years old between 2008 and 2021. Clinical and paraclinical data were retrieved from medical records.
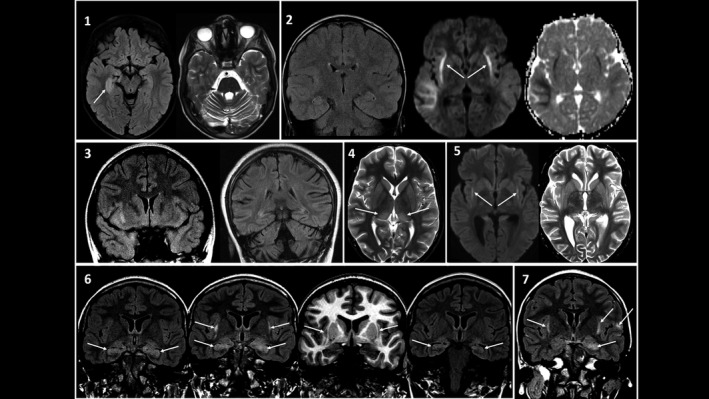
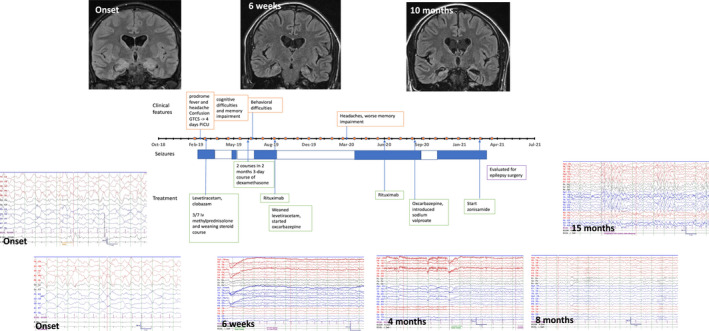
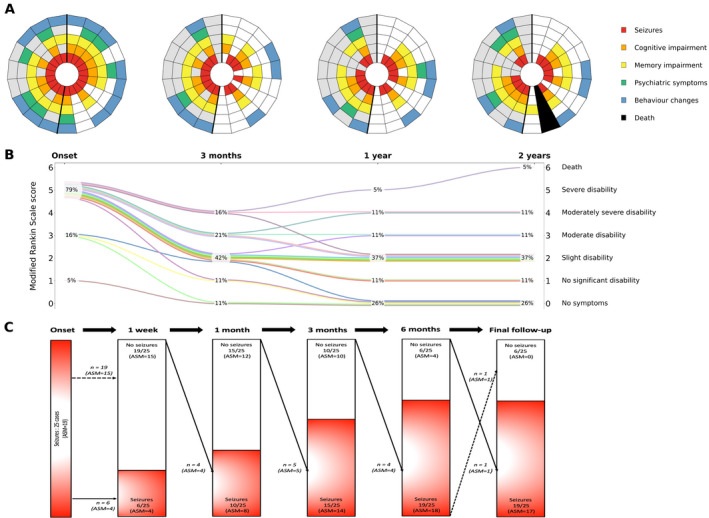
Twenty-five children fulfilling LE criteria were identified, with median age of 11 years (IQR 8, 14) and median follow-up of 24 months (IQR 18, 48). All children presented with seizures; 15/25 (60%) were admitted to intensive care. Neuroimaging demonstrated asymmetric mesial temporal changes in 8/25 (32%), and extra-limbic changes with claustrum involvement in 9/25 (38%). None were positive for LGI1/CASPR2 antibodies (Abs), 2/25 were positive for serum anti-NMDAR Abs, and 2/15 positive for anti-Hu Abs; one died from relapsing neuroblastoma. Two children had serum and CSF anti-GAD antibodies. Initial immune therapy included steroids in 23/25 (92%), intravenous immunoglobulin (IVIg) in 14/25 (56%), and plasma exchange in 7/25 (28%). The commonest second-line treatment was rituximab in 15/25 (60%). Median duration of hospital admission was 21 days (IQR 11, 30). At last follow-up, 13/25 (52%) had refractory seizures and 16/25 (64%) had memory impairment. Six children (24%) had modified Rankin Scale (mRS) scores ≥3. There was no significant difference in mRS, or long-term cognitive and epilepsy outcomes in those who received rituximab versus those who did not.
A diagnosis of autoimmune LE was associated with significant morbidity and adverse outcomes in this pediatric cohort.
描述儿科自身免疫性边缘叶脑炎(LE)的临床特征、检查、治疗和疾病进程。
本研究为回顾性观察性研究,我们从英国儿童神经炎性疾病网络中,选取了 2008 年至 2021 年间 6 家三级中心诊断为 LE 的<18 岁儿童。从病历中提取临床和辅助检查数据。
共纳入 25 名符合 LE 标准的患儿,中位年龄为 11 岁(IQR 8,14),中位随访时间为 24 个月(IQR 18,48)。所有患儿均有癫痫发作,15/25(60%)患儿入住重症监护病房。神经影像学检查显示 8/25(32%)患儿存在不对称性内侧颞叶改变,9/25(38%)患儿存在边缘外改变伴豆状核受累。25 名患儿中无一例抗 LGI1/CASPR2 抗体(Abs)阳性,2/25 例血清抗 NMDAR Abs 阳性,2/15 例抗 Hu Abs 阳性,1 例因复发性神经母细胞瘤死亡。2 例患儿血清和脑脊液抗 GAD 抗体阳性。初始免疫治疗包括 23/25(92%)例患儿使用类固醇,14/25(56%)例患儿使用静脉注射免疫球蛋白(IVIg),7/25(28%)例患儿使用血浆置换。最常见的二线治疗药物为利妥昔单抗,共 15/25(60%)例患儿使用。中位住院时间为 21 天(IQR 11,30)。末次随访时,13/25(52%)例患儿癫痫发作仍未控制,16/25(64%)例患儿存在记忆障碍。6 例患儿(24%)改良 Rankin 量表(mRS)评分≥3 分。在接受利妥昔单抗治疗和未接受治疗的患儿中,mRS 评分、长期认知和癫痫结局无显著差异。
在本儿科队列中,自身免疫性 LE 的诊断与显著的发病率和不良结局相关。