From the Department of Neurology (R.B.P., S.L.A.-P., J.A.d.P.) and Department of Radiology (INRAD) (C.d.M.R.), Hospital das Clínicas, Faculty of Medicine, University of São Paulo (HCFMUSP), Brazil; Queen Square MS Centre (Y.H., O.C.), UCL Institute of Neurology, Faculty of Brain Sciences, University College London; Department of Paediatric Neurology (Y.H., C.H.), Great Ormond Street Hospital for Children, London, United Kingdom; Assistance Publue-Hôpitaux de Paris (E.Y., K.D.), University Hospitals Paris South, Bicêtre Hospital, Le Kremlin Bicêtre, France; Neuroimmunology Program (T.A.) and Neurology Service (A.S.), Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Hospital Clínic, and Pediatric Neuroimmunology Unit (T.A.), Sant Joan de Deu (SJD) Children's Hospital, Universitat de Barcelona, Spain; Department of Neurology (A.B., R.N.), Erasmus University Medical Center, Rotterdam, the Netherlands; Division of Paediatric Neurology (C.L., M.B.), Department of Pediatrics I, Medical University of Innsbruck, Austria; Medical Center of Physical Therapy and Pain Medicine INNOVO (Y.M.), Lviv, Ukraine; Division of Pediatric Neurology (M.B.), Department of Pediatrics and Adolescent Medicine, and Department of Neurology (B.K.), Medical University of Vienna, Austria; Pediatric Neurology (E.W.), Birmingham Women and Children's Hospital, United Kingdom; Department of Neuroscience (L.P.), Pediatric Multiple Sclerosis Center, Bambino Gesù Children Hospital, IRCCS, Rome, Italy; Department of Neurology (M.C.) and Regional Multiple Sclerosis Centre (M.C.), University Hospital San Luigi Gonzaga, Orbassano, Italy; Department of Pediatric Neurology (K.R.), Vestische Kinder und Jugendklinik, Witten/Herdecke University, Datteln, Germany; Children's Neurosciences (M.L.), Evelina London Children's Hospital at Guy's and St Thomas' NHS Foundation Trust, King's Health Partners Academic Health Science Centre; Faculty of Life Sciences and Medicine (M.L.), King's College Hospital, London, United Kingdom; Neurology Department (R.M.), Hôpital Neurologique Pierre Wertheimer, Hospices Civils de Lyon; French Reference Network of Rare Inflammatory Brain and Spinal Diseases (R.M., K.D.), Le Kremlin Bicêtre, France; School of Medicine (D.K.S.), Brain Institute of Rio Grande do Sul (Brains), Pontifical Catholic University of Rio Grande Do Sul (PUCRS), Porto Alegre, Brazil; and Inserm UMR 1184 (K.D.), Immunology of Viral Infections and Autoimmune Diseases, CEA, IDMIT, Le Kremlin Bicêtre, France.
Neurol Neuroimmunol Neuroinflamm. 2020 Jul 30;7(5). doi: 10.1212/NXI.0000000000000837. Print 2020 Sep.
To describe the clinical phenotypes, treatment response, and outcome of children with antibodies against aquaporin-4 (AQP4-Ab) neuromyelitis optica spectrum disorder (NMOSD).
Retrospective, multicenter, and multinational study of patients with AQP4-Ab NMOSD aged <18 years at disease onset from a center in Brazil and 13 European centers. Data on demographics, clinical findings, and laboratory results were analyzed; calculation of annualized relapse rates (ARRs) pre- and on-treatment with disease-modifying therapies (DMTs) and of ORs for predictors of poor outcome was performed.
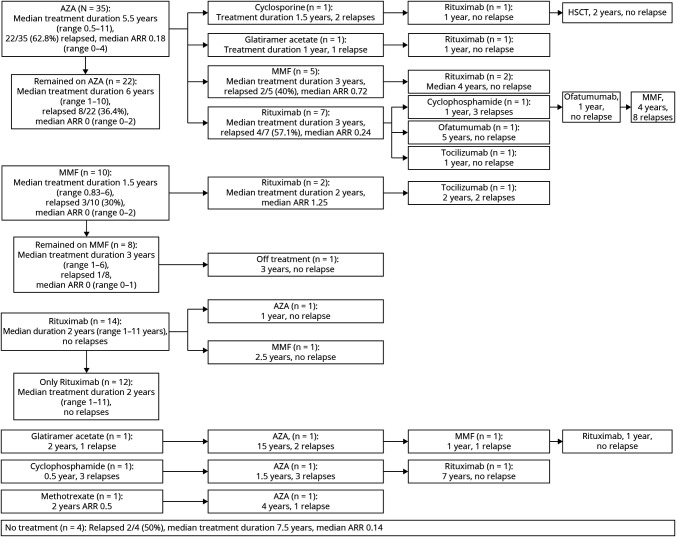
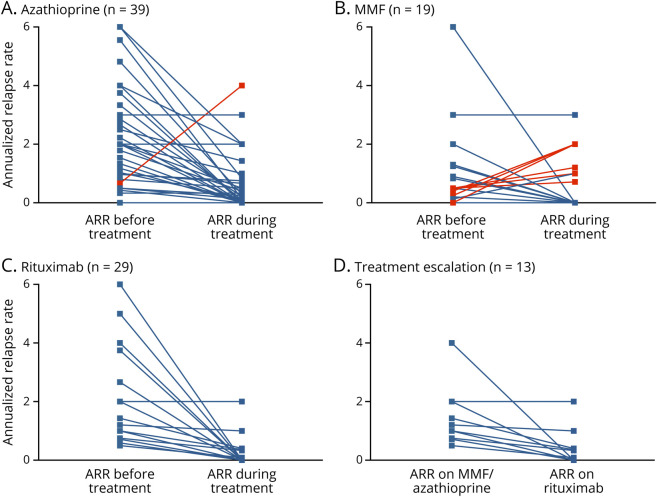
A total of 67 children were identified. At last follow-up (median 4 years, interquartile range 2-10 years), 37/67(57.8%) were found to have permanent disability. A more severe disease course was seen in the non-White ethnicity with both a shorter time to first relapse ( = 0.049) and a worse Expanded Disability Status Scale score at last follow-up ( = 0.008). The median ARR on treatment was 0.18 on azathioprine (n = 39, range 0-4), 0 on mycophenolate mofetil (n = 18, range 0-3), and 0 on rituximab (n = 29, range 0-2). No patient treated with rituximab as first-line therapy relapsed. Optic neuritis at onset was associated with a poor visual outcome below 20/200 (OR 8.669, 95% CI 1.764-42.616, = 0.008), and a younger age at onset was associated with cognitive impairment (OR 0.786, 95% CI 0.644-0.959, = 0.018).
AQP4-Ab NMOSD in children is an aggressive disease with permanent disabilities observed in over half the cohort. All DMTs were associated with a reduction of ARR. First-line rituximab prevented further clinical relapses. International consensus on treatment protocols for children is required to reduce heterogeneity of treatment regimens used worldwide.
This study provides Class IV evidence that for children with AQP4-Ab NMOSD, all DMTs, particularly first-line rituximab, reduced the ARR and prevented further clinical relapses.
描述抗水通道蛋白 4(AQP4-Ab)视神经脊髓炎谱系障碍(NMOSD)患儿的临床表型、治疗反应和结局。
对巴西一家中心和 13 家欧洲中心的发病年龄<18 岁的 AQP4-Ab NMOSD 患儿进行回顾性、多中心、多国研究。分析人口统计学、临床发现和实验室结果;计算疾病修正治疗(DMT)前和治疗期间的年化复发率(ARR),以及预测不良结局的比值比(ORs)。
共纳入 67 例患儿。末次随访(中位数 4 年,四分位距 2-10 年)时,37/67(57.8%)患儿存在永久性残疾。非白种人种族的疾病病程更严重,首次复发的时间更短( = 0.049),末次随访时扩展残疾状况量表评分更差( = 0.008)。阿扎胞苷治疗时的中位 ARR 为 0.18(n = 39,范围 0-4),霉酚酸酯治疗时为 0(n = 18,范围 0-3),利妥昔单抗治疗时为 0(n = 29,范围 0-2)。没有患者在利妥昔单抗作为一线治疗时复发。发病时视神经炎与低于 20/200 的视力不良结局相关(OR 8.669,95%CI 1.764-42.616, = 0.008),发病年龄较小与认知障碍相关(OR 0.786,95%CI 0.644-0.959, = 0.018)。
儿童 AQP4-Ab NMOSD 是一种侵袭性疾病,超过一半的患儿存在永久性残疾。所有 DMT 均与 ARR 降低相关。一线利妥昔单抗可预防进一步的临床复发。需要制定针对儿童的国际治疗方案共识,以减少全球治疗方案的异质性。
本研究提供 IV 级证据表明,对于 AQP4-Ab NMOSD 患儿,所有 DMT,特别是一线利妥昔单抗,均降低了 ARR,预防了进一步的临床复发。