Abdallah Nadine H, Binder Moritz, Rajkumar S Vincent, Greipp Patricia T, Kapoor Prashant, Dispenzieri Angela, Gertz Morie A, Baughn Linda B, Lacy Martha Q, Hayman Suzanne R, Buadi Francis K, Dingli David, Go Ronald S, Hwa Yi L, Fonder Amie L, Hobbs Miriam A, Lin Yi, Leung Nelson, Kourelis Taxiarchis, Warsame Rahma, Siddiqui Mustaqeem A, Kyle Robert A, Bergsagel P Leif, Fonseca Rafael, Ketterling Rhett P, Kumar Shaji K
Division of Hematology, Mayo Clinic, Rochester, MN, USA.
Department of Laboratory Medicine and Pathology, Rochester, MN, USA.
Blood Cancer J. 2022 Jan 31;12(1):21. doi: 10.1038/s41408-022-00611-x.
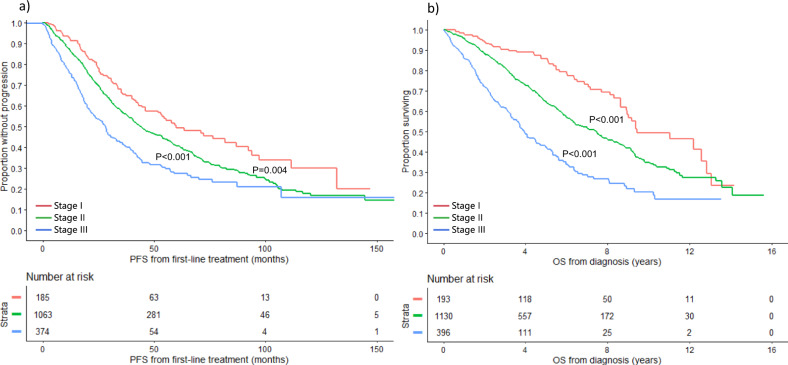
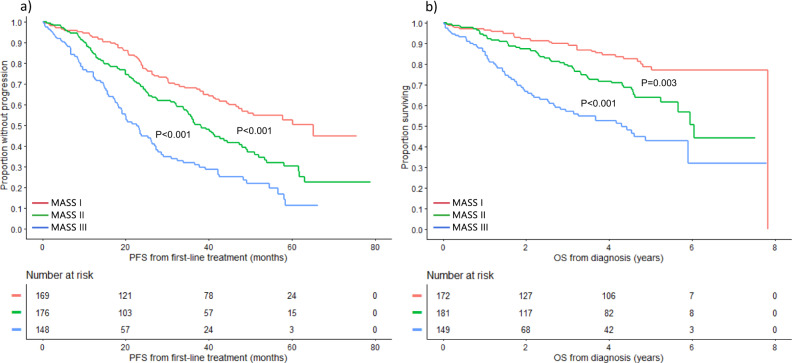
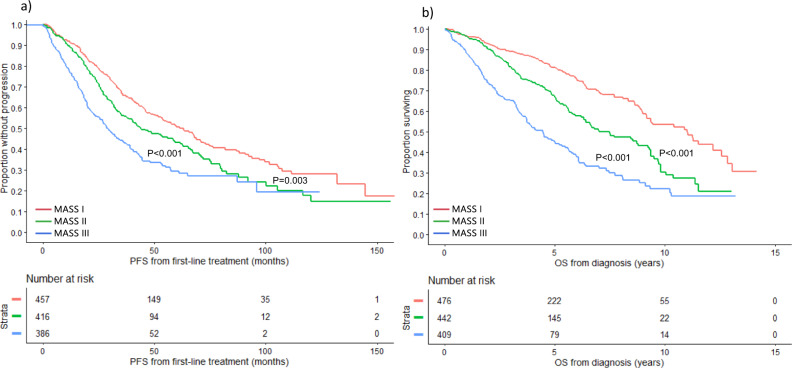
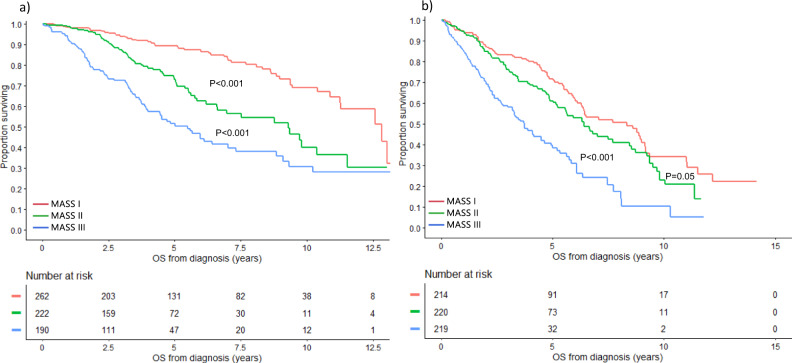
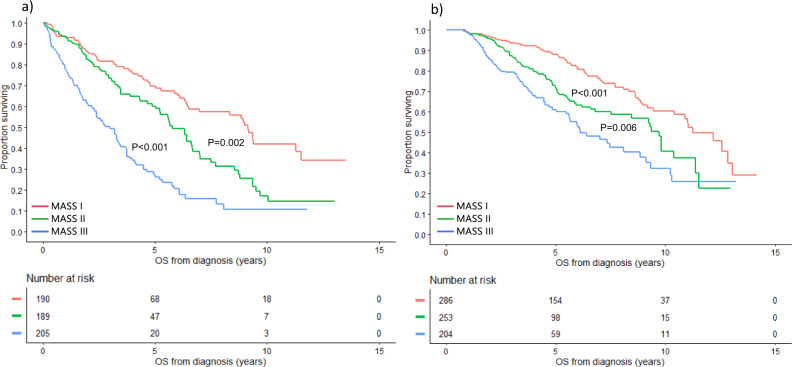
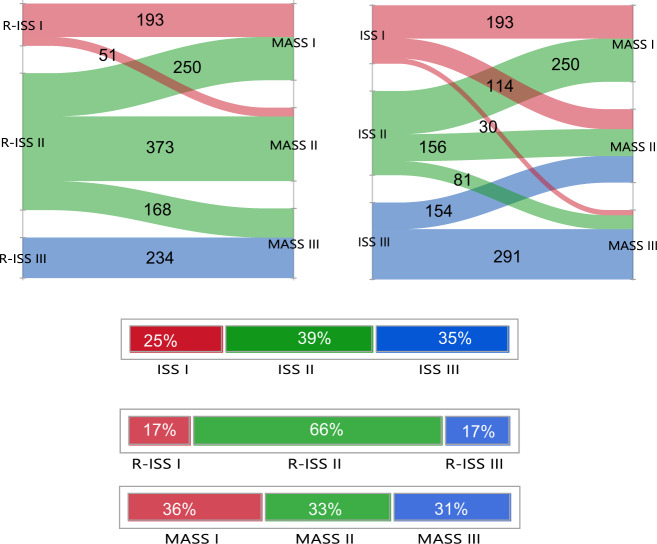
Risk stratification in multiple myeloma is important for prognostication, patient selection for clinical trials, and comparison of treatment approaches. We developed and validated a staging system that incorporates additional FISH abnormalities not included in the R-ISS and reflects the additive effects of co-occurring high-risk disease features. We first evaluated the prognostic value of predefined cytogenetic and laboratory abnormalities in 2556 Mayo Clinic patients diagnosed between February 2004 and June 2019. We then used data from 1327 patients to develop a risk stratification model and validated this in 502 patients enrolled in the MMRF CoMMpass study. On multivariate analysis, high-risk IgH translocations [risk ratio (RR): 1.7], 1q gain/amplification (RR: 1.4), chromosome17 abnormalities (RR: 1.6), ISS III (RR: 1.7), and elevated LDH (RR: 1.3) were independently associated with decreased overall survival (OS). Among 1327 evaluable patients, OS was 11.0 (95% CI: 9.2-12.6), 7.0 (95% CI: 6.3-9.2), and 4.5 (95% CI: 3.7-5.2) years in patients with 0 (stage I), 1 (stage II), and ≥2 (stage III) high-risk factors, respectively. In the MMRF cohort, median OS was 7.8 (95% CI: NR-NR), 6.0 (95% CI: 5.7-NR), and 4.3 (95% CI: 2.7-NR) years in the 3 groups, respectively (P < 0.001). This 5-factor, 3-tier system is easy to implement in practice and improves upon the current R-ISS.
多发性骨髓瘤的风险分层对于预后评估、临床试验患者选择以及治疗方法比较至关重要。我们开发并验证了一种分期系统,该系统纳入了R-ISS中未包含的其他荧光原位杂交(FISH)异常情况,并反映了同时出现的高危疾病特征的累加效应。我们首先评估了2004年2月至2019年6月在梅奥诊所诊断的2556例患者中预定义的细胞遗传学和实验室异常的预后价值。然后,我们使用1327例患者的数据建立了一个风险分层模型,并在参加MMRF CoMMpass研究的502例患者中进行了验证。多因素分析显示,高危免疫球蛋白重链(IgH)易位[风险比(RR):1.7]、1q增益/扩增(RR:1.4)、17号染色体异常(RR:1.6)、国际分期系统(ISS)III期(RR:1.7)和乳酸脱氢酶(LDH)升高(RR:1.3)与总生存期(OS)缩短独立相关。在1327例可评估患者中,0个(I期)、1个(II期)和≥2个(III期)高危因素患者的OS分别为11.0(95%置信区间:9.2 - 12.6)年、7.0(95%置信区间:6.3 - 9.2)年和4.5(95%置信区间:3.7 - 5.2)年。在MMRF队列中,三组患者的中位OS分别为7.8(95%置信区间:未报告 - 未报告)年、6.0(95%置信区间:5.7 - 未报告)年和4.3(95%置信区间:2.7 - 未报告)年(P < 0.001)。这个五因素、三层系统在实践中易于实施,并且对当前的R-ISS进行了改进。