Stephenson Cardiac Imaging Centre, Libin Cardiovascular Institute of Alberta, University of Calgary, #0700, SSB, Foothills Medical Centre, 1403-29th St. NW, Calgary, AB, T2N2T9, Canada.
Department of Cardiac Sciences, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada.
Sci Rep. 2022 Feb 2;12(1):1739. doi: 10.1038/s41598-022-05790-y.
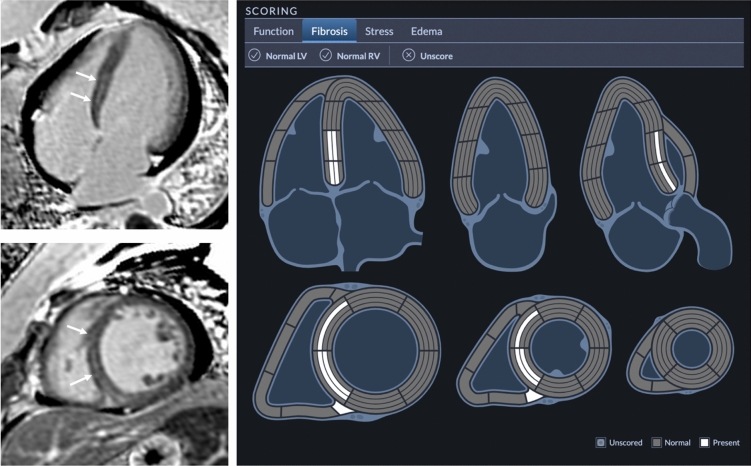
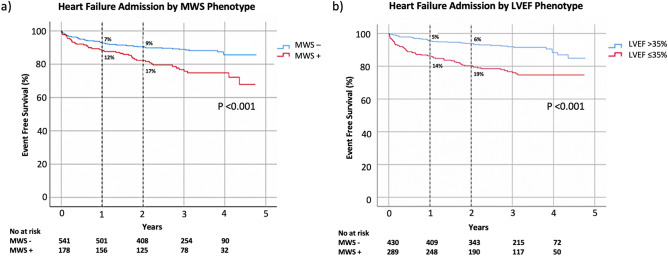
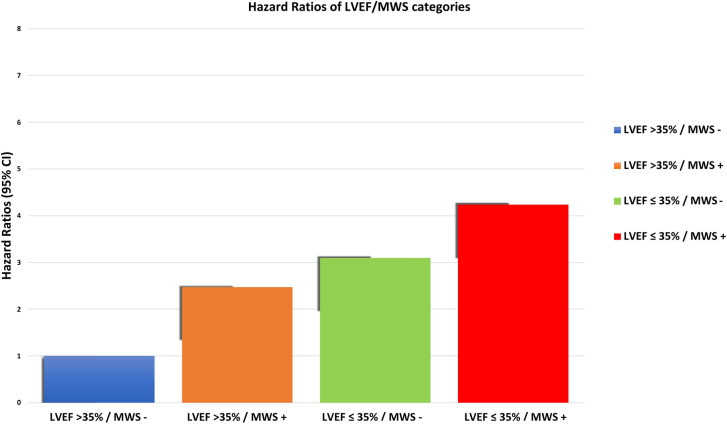
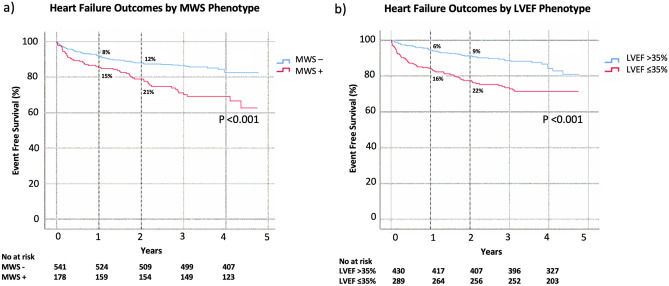
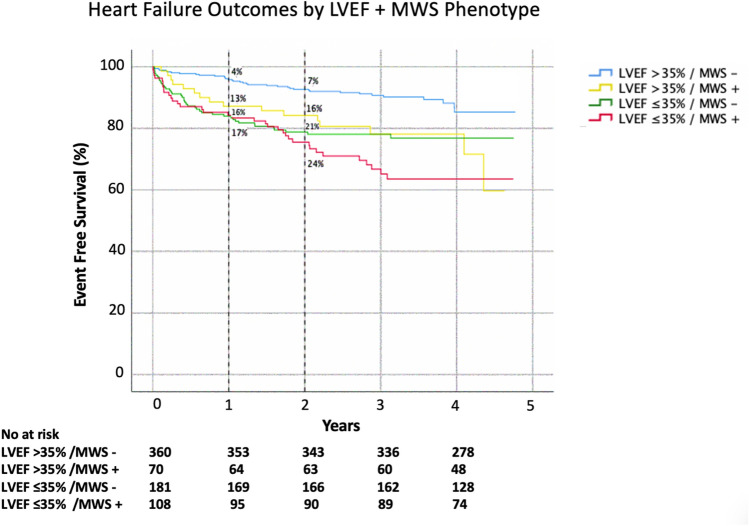
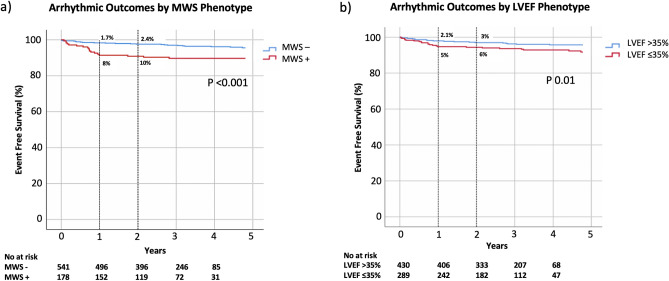
Heart failure (HF) admission is a dominant contributor to morbidity and healthcare costs in dilated cardiomyopathy (DCM). Mid-wall striae (MWS) fibrosis by late gadolinium enhancement (LGE) imaging has been associated with elevated arrhythmia risk. However, its capacity to predict HF-specific outcomes is poorly defined. We investigated its role to predict HF admission and relevant secondary outcomes in a large cohort of DCM patients. 719 patients referred for LGE MRI assessment of DCM were enrolled and followed for clinical events. Standardized image analyses and interpretations were conducted inclusive of coding the presence and patterns of fibrosis observed by LGE imaging. The primary clinical outcome was hospital admission for decompensated HF. Secondary heart failure and arrhythmic composite endpoints were also studied. Median age was 57 (IQR 47-65) years and median LVEF 40% (IQR 29-47%). Any fibrosis was observed in 228 patients (32%) with MWS fibrosis pattern present in 178 (25%). At a median follow up of 1044 days, 104 (15%) patients experienced the primary outcome, and 127 (18%) the secondary outcome. MWS was associated with a 2.14-fold risk of the primary outcome, 2.15-fold risk of the secondary HF outcome, and 2.23-fold risk of the secondary arrhythmic outcome. Multivariable analysis adjusting for all relevant covariates, inclusive of LVEF, showed patients with MWS fibrosis to experience a 1.65-fold increased risk (95% CI 1.11-2.47) of HF admission and 1-year event rate of 12% versus 7% without this phenotypic marker. Similar findings were observed for the secondary outcomes. Patients with LVEF > 35% plus MWS fibrosis experienced similar event rates to those with LVEF ≤ 35%. MWS fibrosis is a powerful and independent predictor of clinical outcomes in patients with DCM, identifying patients with LVEF > 35% who experience similar event rates to those with LVEF below this conventionally employed high-risk phenotype threshold.
心力衰竭(HF)入院是扩张型心肌病(DCM)发病率和医疗保健费用的主要原因。晚期钆增强(LGE)成像中的中壁条纹(MWS)纤维化与心律失常风险升高有关。然而,其预测 HF 特异性结局的能力尚未得到明确界定。我们在大量 DCM 患者中研究了其预测 HF 入院和相关次要结局的作用。招募了 719 名接受 LGE MRI 评估 DCM 的患者,并对其进行了临床事件随访。进行了标准化的图像分析和解释,包括对 LGE 成像观察到的纤维化的存在和模式进行编码。主要临床结局为因心力衰竭失代偿而住院。还研究了次要心力衰竭和心律失常复合终点。中位年龄为 57 岁(IQR 47-65 岁),中位 LVEF 为 40%(IQR 29-47%)。228 名患者(32%)存在任何纤维化,178 名患者(25%)存在 MWS 纤维化模式。中位随访时间为 1044 天,104 名患者(15%)发生主要结局,127 名患者(18%)发生次要结局。MWS 与主要结局的风险增加 2.14 倍、次要 HF 结局的风险增加 2.15 倍和次要心律失常结局的风险增加 2.23 倍相关。调整所有相关协变量(包括 LVEF)的多变量分析显示,MWS 纤维化患者 HF 入院的风险增加 1.65 倍(95%CI 1.11-2.47),1 年事件发生率为 12%,而无这种表型标志物的患者为 7%。次要结局也观察到类似的发现。LVEF>35%且存在 MWS 纤维化的患者与 LVEF≤35%的患者具有相似的事件发生率。MWS 纤维化是 DCM 患者临床结局的强大且独立预测因子,确定了 LVEF>35%且具有相似事件发生率的患者与传统高风险表型阈值以下的 LVEF 患者相似。