Abdel-Qadir Husam, Fang Jiming, Lee Douglas S, Tu Jack V, Amir Eitan, Austin Peter C, Anderson Geoffrey M
Department of Medicine, Women's College Hospital, Toronto, ON, Canada (H.A.-Q.).
Division of Cardiology, Peter Munk Cardiac Centre and the Ted Rogers Centre for Heart Research, University Health Network, Toronto, ON, Canada (H.A.-Q., D.S.L.).
Circ Cardiovasc Qual Outcomes. 2018 Jul;11(7):e004580. doi: 10.1161/CIRCOUTCOMES.118.004580.
Ignoring competing risks in time-to-event analyses can lead to biased risk estimates, particularly for elderly patients with multimorbidity. We aimed to demonstrate the impact of considering competing risks when estimating the cumulative incidence and risk of stroke among elderly atrial fibrillation patients.
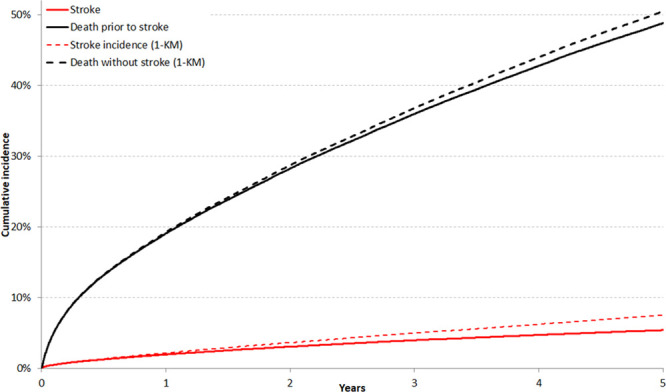
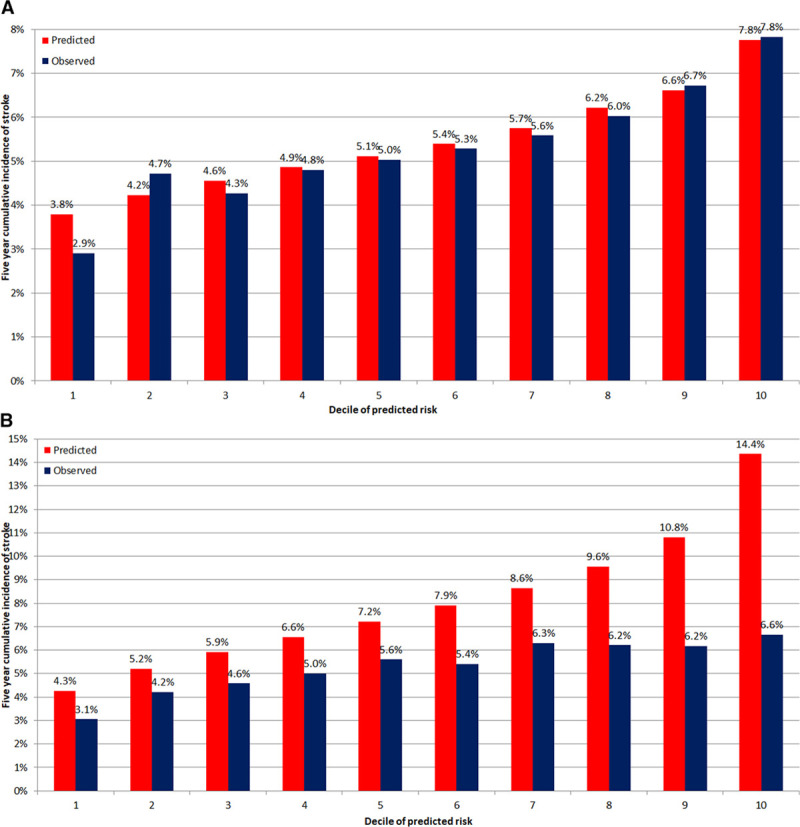
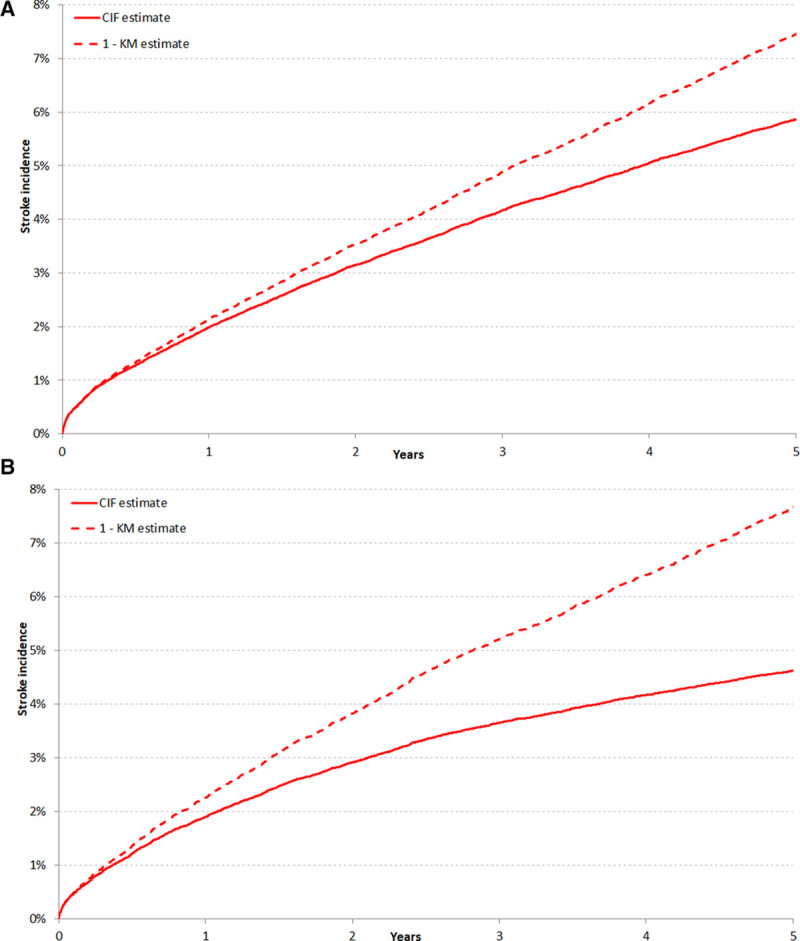
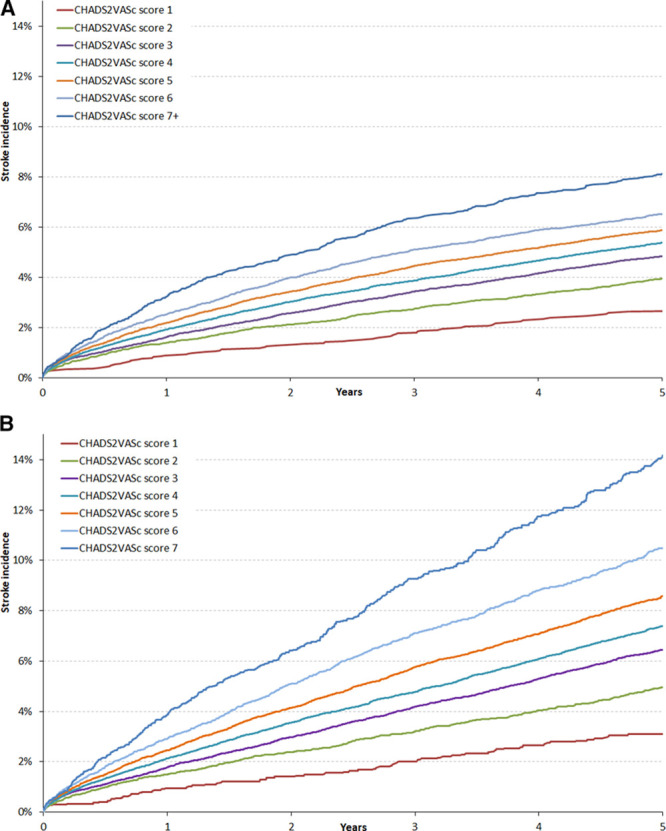
Using linked administrative databases, we identified patients with atrial fibrillation aged ≥66 years discharged from hospital in ON, Canada between January 1, 2007, and March 31, 2011. We estimated the cumulative incidence of stroke hospitalization using the complement of the Kaplan-Meier function and the cumulative incidence function. This was repeated after stratifying the cohort by presence of prespecified comorbidities: chronic kidney disease, chronic obstructive pulmonary disease, cancer, or dementia. The full cohort was used to regress components of the CHADSVASc (congestive heart failure, hypertension, age, diabetes mellitus, stroke, vascular disease, sex) score on the hazard of stroke hospitalization using the Fine-Gray and Cox methods. These models were subsequently used to predict the 5-year risk of stroke hospitalization. Among 136 156 patients, the median CHADSVASc score was 4 and 84 728 patients (62.2%) had ≥1 prespecified comorbidity. The 5-year cumulative incidence of stroke was 5.4% (95% confidence interval, 5.3%-5.5%), whereas that of death without stroke was 48.8% (95% confidence interval, 48.5%-49.1%). The incidence of both events was overestimated by the Kaplan-Meier method; stroke incidence was overestimated by a relative factor of 39%. The degree of overestimation was larger among patients with non-CHADSVASc comorbidity because of higher incidence of death without stroke. The Fine-Gray model demonstrated better calibration than the Cox model, which consistently overpredicted stroke incidence.
The incidence of death without stroke was 9-fold higher than that of stroke, leading to biased estimates of stroke risk with traditional time-to-event methods. Statistical methods that appropriately account for competing risks should be used to mitigate this bias.
在事件发生时间分析中忽略竞争风险可能导致风险估计有偏差,对于患有多种疾病的老年患者尤其如此。我们旨在证明在估计老年房颤患者中风的累积发病率和风险时考虑竞争风险的影响。
利用关联的行政数据库,我们确定了2007年1月1日至2011年3月31日期间在加拿大安大略省出院的年龄≥66岁的房颤患者。我们使用Kaplan-Meier函数的互补函数和累积发病率函数估计中风住院的累积发病率。在按预先指定的合并症(慢性肾病、慢性阻塞性肺疾病、癌症或痴呆症)的存在对队列进行分层后重复此操作。使用Fine-Gray方法和Cox方法,将整个队列用于将CHADSVASc(充血性心力衰竭、高血压、年龄、糖尿病、中风、血管疾病、性别)评分的组成部分回归到中风住院的风险上。这些模型随后用于预测中风住院的5年风险。在136156名患者中,CHADSVASc评分中位数为4,84728名患者(62.2%)有≥1种预先指定的合并症。中风的5年累积发病率为5.4%(95%置信区间,5.3%-5.5%),而无中风死亡的累积发病率为48.8%(95%置信区间,48.5%-49.1%)。Kaplan-Meier方法高估了这两种事件的发病率;中风发病率被高估了39%的相对因子。由于无中风死亡的发生率较高,在患有非CHADSVASc合并症的患者中高估程度更大。Fine-Gray模型显示出比Cox模型更好的校准,Cox模型一直高估中风发病率。
无中风死亡的发病率比中风发病率高9倍,导致传统事件发生时间方法对中风风险的估计有偏差。应使用适当考虑竞争风险的统计方法来减轻这种偏差。