Maniam Anita, Chee Min Lim, Kiet Phang Ling, Vendargon Francesca Martina, Othman Othmaliza
Ophthalmology, Universiti Kebangsaan Malaysia Medical Centre, Cheras, MYS.
Ophthalmology, Hospital Sultanah Aminah, Johor Bahru, MYS.
Cureus. 2021 Dec 28;13(12):e20769. doi: 10.7759/cureus.20769. eCollection 2021 Dec.
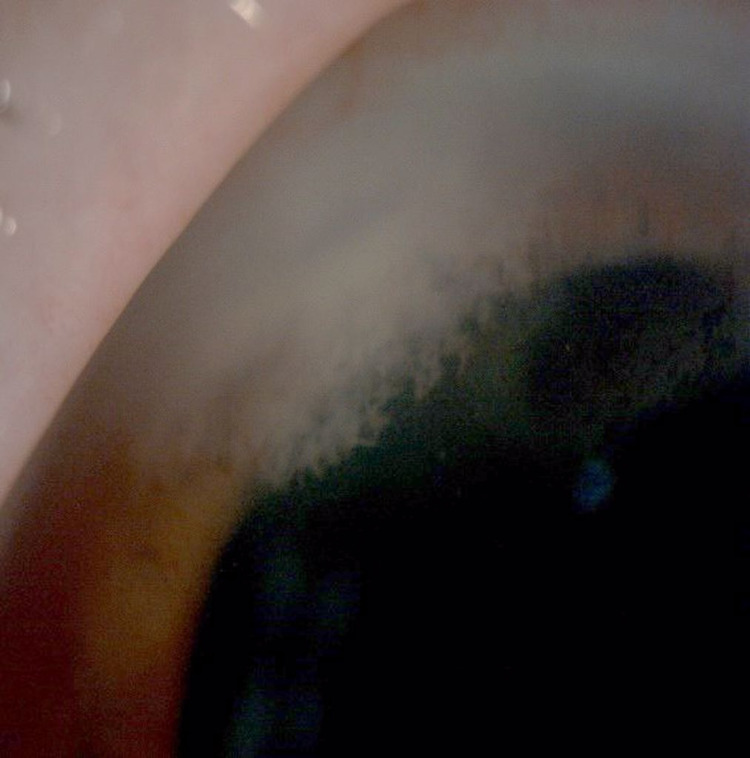
Keratomycosis is a significant cause of mono-ocular blindness, especially in tropical regions. Fungal keratitis developing in corneal incisions is very rare. We report the experience of treating two patients diagnosed with recalcitrant candida keratitis post-phacoemulsification with anterior chamber washout and deep debridement. The first patient was a 68-year-old woman who underwent left eye phacoemulsification nine months ago with a postoperative best corrected visual acuity of 6/6. The second patient was a 73-year-old man who had uneventful right eye phacoemulsification six months prior with a postoperative best corrected visual acuity of 6/9. Both patients used topical steroids postoperatively for more than three months and noted a drop in vision. Both patients had deep stromal infiltration and endothelial plaque at the primary corneal wound. They were unresponsive to topical, intracameral, and systemic antifungal therapy. Both patients underwent anterior chamber evacuation of hypopyon and endothelial plaque removal. Evacuation of hypopyon and removal of endothelial plaque was done with a 23G vitrectomy cutter using a low-powered vacuum controlled at 200 mmHg. The fluid inside the tubing was sent for culture analysis. We used viscoelastic coating on the endothelium to minimize the damage during the operations. Intracameral amphotericin B 15 µg/0.1 ml was given at the end of the operation. Postoperatively, both patients had clear corneas. The first patient's visual acuity improved 6/18, and the second patient's visual acuity improved to 6/9. Both cultures isolated sensitive to amphotericin. These patient cases highlight that evacuation of the anterior chamber infiltration in recalcitrant fungal keratitis and intracameral injection of amphotericin B can be an effective adjuvant therapy.
角膜真菌病是单眼失明的一个重要原因,尤其是在热带地区。角膜切口处发生的真菌性角膜炎非常罕见。我们报告了两例经前房冲洗和深层清创术治疗的白内障超声乳化术后顽固性念珠菌性角膜炎患者的治疗经验。第一例患者是一名68岁女性,九个月前接受了左眼白内障超声乳化术,术后最佳矫正视力为6/6。第二例患者是一名73岁男性,六个月前右眼白内障超声乳化术顺利,术后最佳矫正视力为6/9。两名患者术后均使用局部类固醇超过三个月,并注意到视力下降。两名患者在原角膜伤口处均有深层基质浸润和内皮斑块。他们对局部、前房内和全身抗真菌治疗均无反应。两名患者均接受了前房积脓清除和内皮斑块清除。使用23G玻璃体切割器以200 mmHg的低功率真空进行前房积脓清除和内皮斑块清除。将管道内的液体送去进行培养分析。我们在手术过程中在内皮上使用粘弹剂涂层以尽量减少损伤。手术结束时给予前房内两性霉素B 15 µg/0.1 ml。术后,两名患者的角膜均清晰。第一例患者的视力提高到6/18,第二例患者的视力提高到6/9。两种培养物均分离出对两性霉素敏感的菌株。这些病例表明,顽固性真菌性角膜炎的前房浸润清除和前房内注射两性霉素B可以是一种有效的辅助治疗方法。