Division of Cancer Epidemiology and Genetics, National Cancer Institute, Rockville, Maryland, USA.
Slone Epidemiology Center, Boston University, Boston, Massachusetts, USA.
Hepatology. 2022 Sep;76(3):589-598. doi: 10.1002/hep.32394. Epub 2022 Apr 22.
HCC is characterized by racial/ethnic disparities in rates. Recent USA reports suggest that incidence has begun to decline, but it is not clear whether the declines have occurred among all groups, nor whether mortality has declined. Thus, the current study examined USA incidence and mortality between 1992 and 2018.
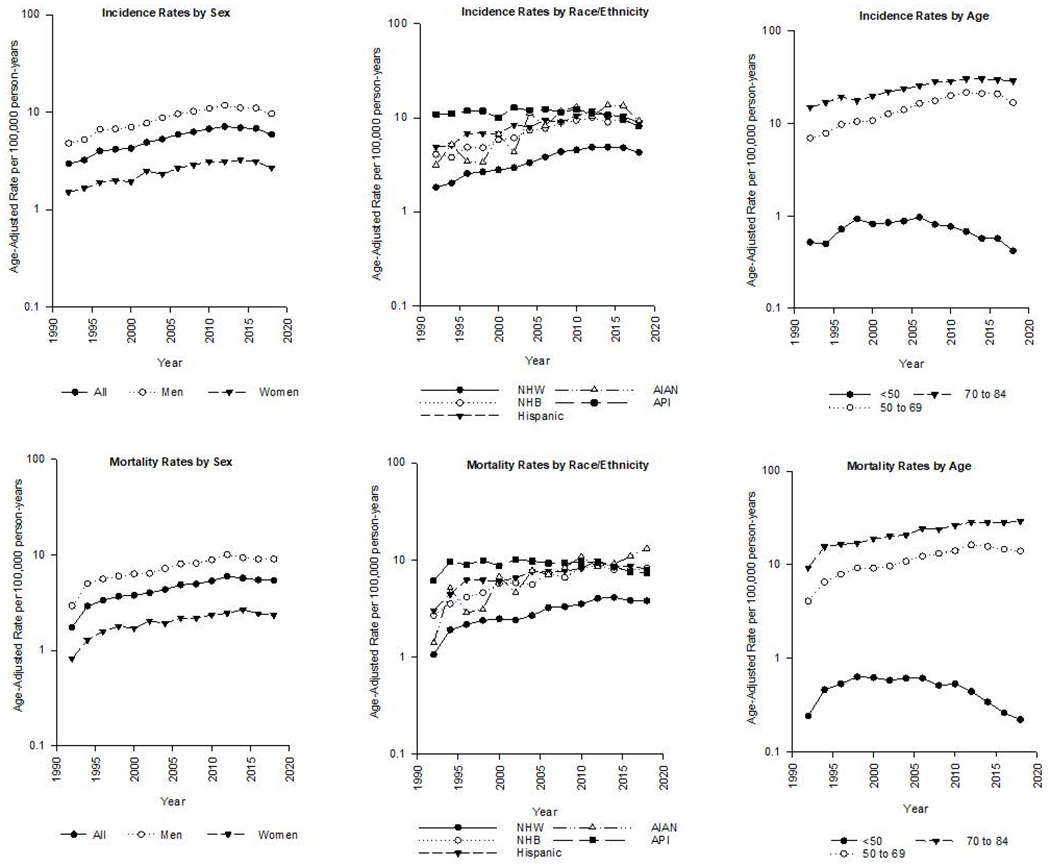
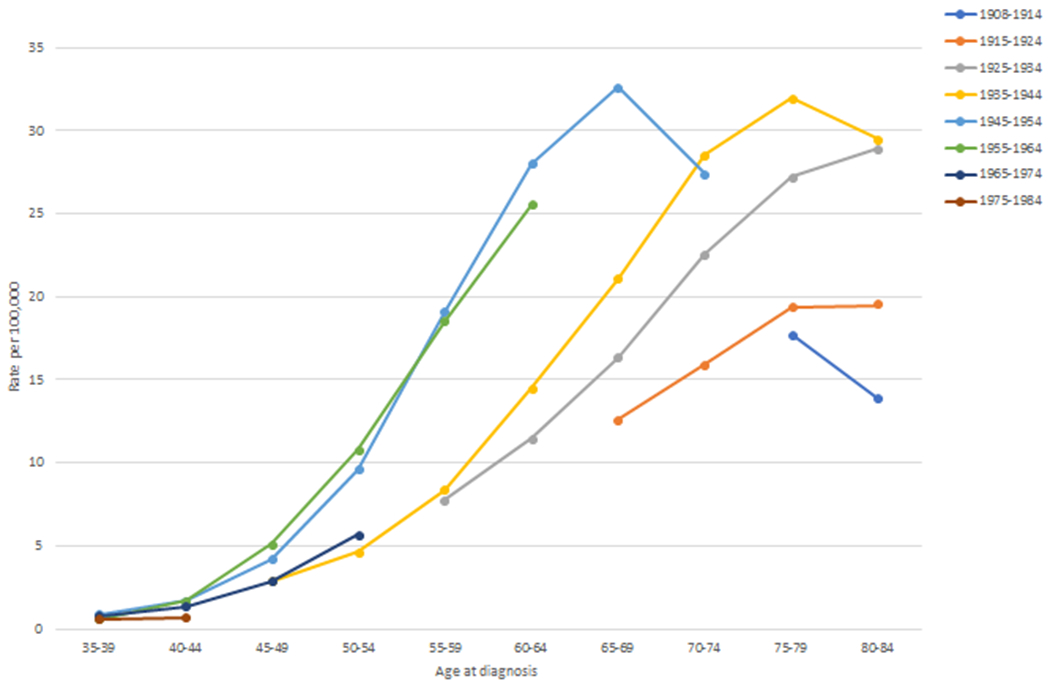
APPROACH & RESULTS: HCC incidence and incidence-based mortality data from the Surveillance, Epidemiology, and End Results program were used to calculate age-standardized rates by race/ethnicity, sex, and age. Trends were analyzed using joinpoint regression to estimate annual percent change (APC). Age-period-cohort models assessed the effects on trends of age, calendar period, and birth cohort. Overall, HCC incidence significantly declined between 2015 and 2018 (APC, -5.6%). Whereas most groups experienced incidence declines, the trends were most evident among Asians/Pacific Islanders, women, and persons <50 years old. Exceptions were the rates among non-Hispanic Black persons, which did not significantly decline (APC, -0.7), and among American Indians/Alaska Natives, which significantly increased (APC, +4.3%). Age-period-cohort modeling found that birth cohort had a greater effect on rates than calendar period. Among the baby boom cohorts, the 1950-1954 cohort had the highest rates. Similar to the overall incidence decline, HCC mortality rates declined between 2013 and 2018 (APC, -2.2%).
HCC incidence and mortality rates began to decline for most groups in 2015, but persistent differences in rates continued to exist. Rates among non-Hispanic Black persons did not decline significantly, and rates among American Indians/Alaska Natives significantly increased, suggesting that greater effort is needed to reduce the HCC burden among these vulnerable groups.
肝癌的发病率存在种族/民族差异。最近美国的报告表明,发病率已经开始下降,但目前尚不清楚这些下降是否发生在所有人群中,也不清楚死亡率是否有所下降。因此,本研究调查了 1992 年至 2018 年期间美国肝癌的发病率和死亡率。
利用监测、流行病学和最终结果计划中的肝癌发病率和基于发病率的死亡率数据,按种族/族裔、性别和年龄计算年龄标准化率。使用 joinpoint 回归分析趋势,估计年变化百分比(APC)。年龄-时期-队列模型评估了年龄、日历时期和出生队列对趋势的影响。总体而言,2015 年至 2018 年间肝癌发病率显著下降(APC,-5.6%)。虽然大多数人群的发病率都有所下降,但这种趋势在亚洲/太平洋岛民、女性和<50 岁人群中最为明显。非西班牙裔黑人群体的发病率没有显著下降(APC,-0.7%),而美洲印第安人/阿拉斯加原住民的发病率显著上升(APC,+4.3%)是例外。年龄-时期-队列模型发现,出生队列对发病率的影响大于日历时期。在生育高峰期的队列中,1950-1954 年出生的队列发病率最高。与整体发病率下降相似,2013 年至 2018 年间肝癌死亡率也有所下降(APC,-2.2%)。
大多数人群的肝癌发病率和死亡率从 2015 年开始下降,但持续存在的发病率差异仍然存在。非西班牙裔黑人群体的发病率没有显著下降,而美洲印第安人/阿拉斯加原住民的发病率显著上升,这表明需要加大努力来降低这些弱势群体的肝癌负担。