Novo Nordisk Foundation Center for Protein Research, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark.
Clinical Pharmacology Unit, Zealand University Hospital, Roskilde, Denmark.
Pharmacoepidemiol Drug Saf. 2022 Jun;31(6):632-642. doi: 10.1002/pds.5415. Epub 2022 Feb 22.
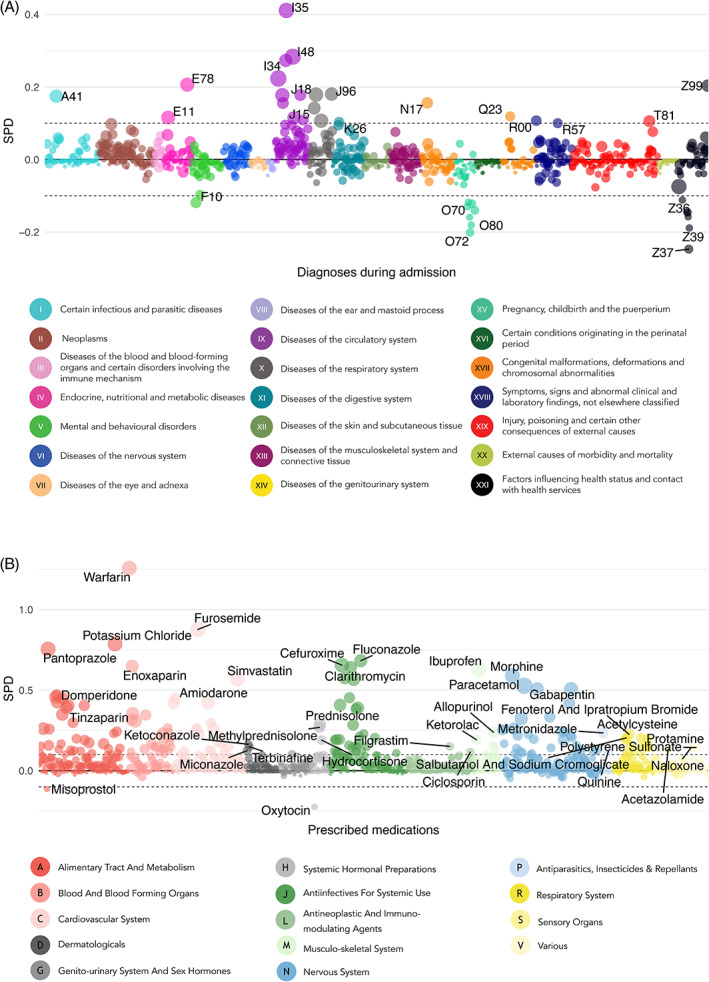
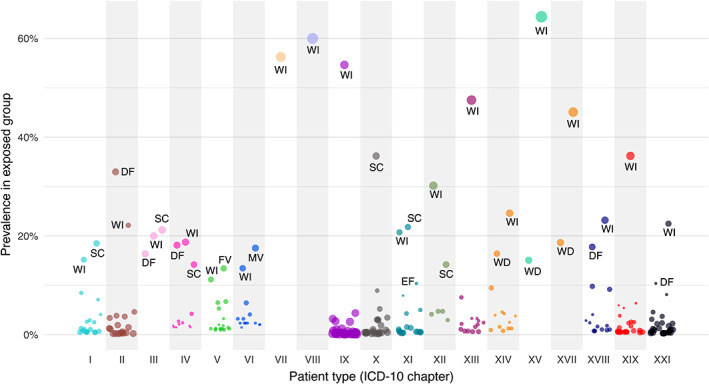
While the beneficial effects of medications are numerous, drug-drug interactions may lead to adverse drug reactions that are preventable causes of morbidity and mortality. Our goal was to quantify the prevalence of potential drug-drug interactions in drug prescriptions at Danish hospitals, estimate the risk of adverse outcomes associated with discouraged drug combinations, and highlight the patient types (defined by the primary diagnosis of the admission) that appear to be more affected.
This cross-sectional (descriptive part) and cohort study (adverse outcomes part) used hospital electronic health records from two Danish regions (~2.5 million people) from January 2008 through June 2016. We included all inpatients receiving two or more medications during their admission and considered concomitant prescriptions of potentially interacting drugs as per the Danish Drug Interaction Database. We measured the prevalence of potential drug-drug interactions in general and discouraged drug pairs in particular during admissions and associations with adverse outcomes: post-discharge all-cause mortality rate, readmission rate and length-of-stay.
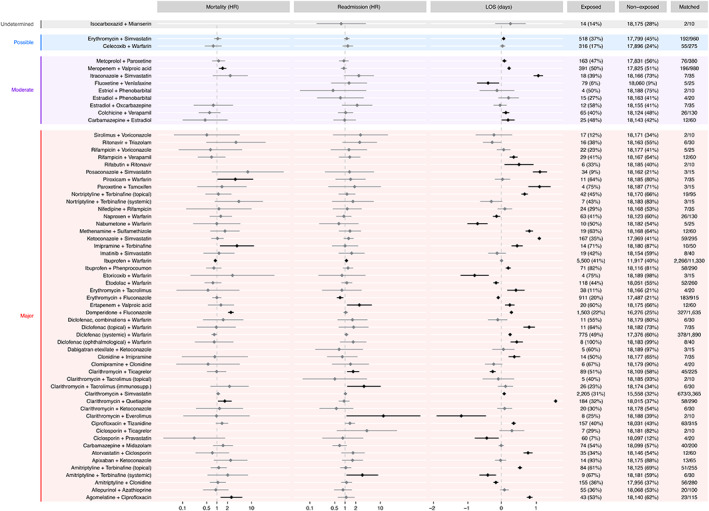
Among 2 886 227 hospital admissions (945 475 patients; median age 62 years [IQR: 41-74]; 54% female; median number of drugs 7 [IQR: 4-11]), patients in 1 836 170 admissions were exposed to at least one potential drug-drug interaction (659 525 patients; median age 65 years [IQR: 49-77]; 54% female; median number of drugs 9 [IQR: 6-13]) and in 27 605 admissions to a discouraged drug pair (18 192 patients; median age 68 years [IQR: 58-77]; female 46%; median number of drugs 16 [IQR: 11-22]). Meropenem-valproic acid (HR: 1.5, 95% CI: 1.1-1.9), domperidone-fluconazole (HR: 2.5, 95% CI: 2.1-3.1), imipramine-terbinafine (HR: 3.8, 95% CI: 1.2-12), agomelatine-ciprofloxacin (HR: 2.6, 95% CI: 1.3-5.5), clarithromycin-quetiapine (HR: 1.7, 95% CI: 1.1-2.7) and piroxicam-warfarin (HR: 3.4, 95% CI: 1-11.4) were associated with elevated mortality. Confidence interval bounds of pairs associated with readmission were close to 1; length-of-stay results were inconclusive.
Well-described potential drug-drug interactions are still missed and alerts at point of prescription may reduce the risk of harming patients; prescribing clinicians should be alert when using strong inhibitor/inducer drugs (i.e. clarithromycin, valproic acid, terbinafine) and prevalent anticoagulants (i.e. warfarin and non-steroidal anti-inflammatory drugs - NSAIDs) due to their great potential for dangerous interactions. The most prominent CYP isoenzyme involved in mortality and readmission rates was 3A4.
尽管药物的有益作用很多,但药物相互作用可能导致可预防的药物不良反应,从而导致发病率和死亡率。我们的目标是量化丹麦医院药物处方中潜在药物相互作用的发生率,估计与不推荐药物组合相关的不良后果风险,并突出受影响的患者类型(根据入院的主要诊断定义)。
本研究采用丹麦两个地区(约 250 万人)的医院电子健康记录进行了横断面(描述性部分)和队列研究(不良后果部分)。我们纳入了所有在住院期间接受两种或多种药物治疗的住院患者,并根据丹麦药物相互作用数据库考虑了潜在相互作用药物的同时处方。我们测量了住院期间潜在药物相互作用的发生率(一般情况)和特别不推荐药物组合的发生率,并与不良后果相关:出院后全因死亡率、再入院率和住院时间。
在 2886227 例住院治疗(945475 名患者;中位年龄 62 岁[IQR:41-74];54%为女性;中位用药数 7[IQR:4-11])中,1836170 例(659525 名患者;中位年龄 65 岁[IQR:49-77];54%为女性;中位用药数 9[IQR:6-13])患者暴露于至少一种潜在药物相互作用,27605 例(18192 名患者;中位年龄 68 岁[IQR:58-77];46%为女性;中位用药数 16[IQR:11-22])患者暴露于一种不推荐药物组合。美罗培南-丙戊酸(HR:1.5,95%CI:1.1-1.9)、多潘立酮-氟康唑(HR:2.5,95%CI:2.1-3.1)、丙咪嗪-特比萘芬(HR:3.8,95%CI:1.2-12)、阿戈美拉汀-环丙沙星(HR:2.6,95%CI:1.3-5.5)、克拉霉素-喹硫平(HR:1.7,95%CI:1.1-2.7)和吡罗昔康-华法林(HR:3.4,95%CI:1-11.4)与死亡率升高相关。与再入院相关的配对置信区间边界接近 1;住院时间结果不确定。
描述良好的潜在药物相互作用仍然被遗漏,处方时的提醒可能会降低伤害患者的风险;当使用强效抑制剂/诱导剂药物(如克拉霉素、丙戊酸、特比萘芬)和常见的抗凝剂(如华法林和非甾体抗炎药-NSAIDs)时,临床医生应保持警惕,因为它们存在很大的危险相互作用风险。与死亡率和再入院率最相关的 CYP 同工酶是 3A4。