MRC Centre for Reproductive Health, The University of Edinburgh, Queen's Medical Research Institute, Edinburgh, UK.
Reprod Fertil. 2021 Feb 26;2(1):C1-C7. doi: 10.1530/RAF-20-0044. eCollection 2021 Jan.
The corpus luteum is the source of progesterone in the luteal phase of the cycle and the initial two-thirds of the first trimester of pregnancy. Normal luteal function is required for fertility and the maintenance of pregnancy. Progesterone administration is increasingly used during fertility treatments and in early pregnancy to mitigate potentially inadequate corpus luteum function. This commentary considers the concept of the inadequate corpus luteum and the role and effects of exogenous progesterone. Progesterone supplementation does have important beneficial effects but we should be wary of therapeutic administration beyond or outside the evidence base.
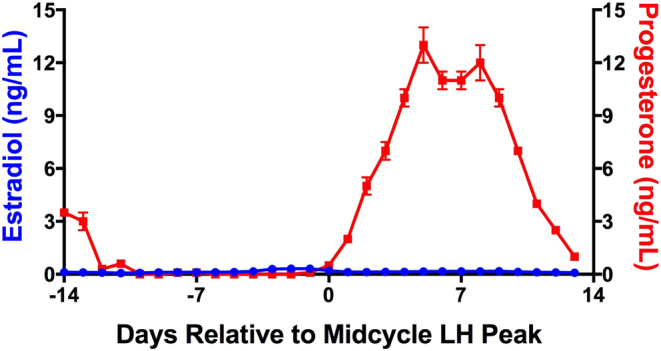
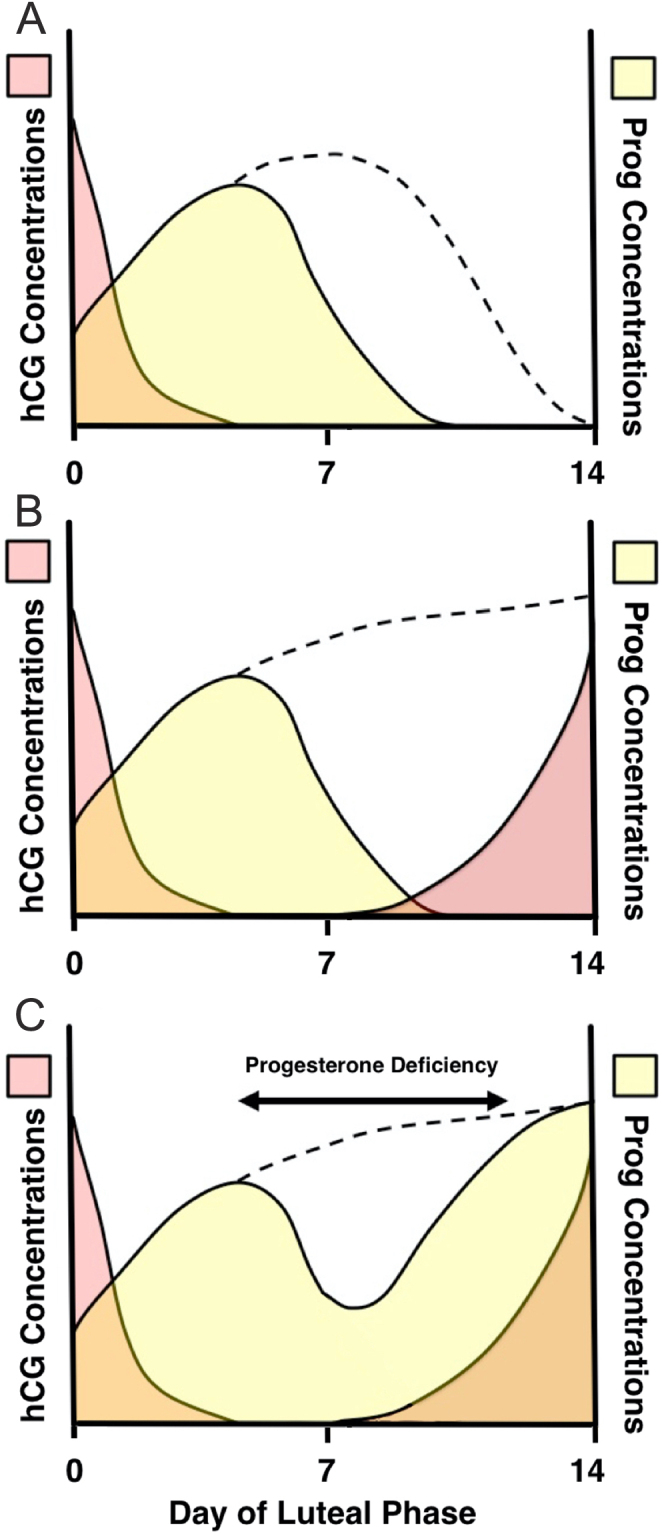
After an egg is released a structure is formed on the ovary called a corpus luteum (CL). This produces a huge amount of a hormone called progesterone. Progesterone makes the womb ready for pregnancy but if a pregnancy does not happen the CL disappears after 12-14 days and this causes a period. If a pregnancy occurs, then the pregnancy hormone (hCG) keeps the CL alive and its progesterone supports the pregnancy for the next 6-8 weeks until the placenta takes over and the corpus luteum disappears. That means that if the CL is not working correctly there could be problems getting pregnant or staying pregnant. If a CL is not producing enough progesterone it usually means there is a problem with the growing or releasing of the egg and treatment should focus on these areas. In IVF cycles, where normal hormones are switched off, the CL does not produce quite enough progesterone before the pregnancy test and extra progesterone is needed at this time. In recurrent or threatened miscarriage, however, there is not any evidence that the CL is not working well or progesterone is low. However, there is benefit in taking extra progesterone if there is bleeding in early pregnancy in women with previous miscarriages. This might be because of the effects of high-dose progesterone on the womb or immune system. As changes to the hormone environment in pregnancy may have some life-long consequences for the offspring we have to be careful only to give extra progesterone when we are sure it is needed.
黄体是周期黄体期和妊娠头三个月前两到三分之二时孕激素的来源。正常黄体功能是生育和妊娠维持所必需的。在生育治疗和早期妊娠中,越来越多地使用孕激素来缓解潜在的黄体功能不足。本评论考虑了黄体功能不足的概念以及外源性孕激素的作用和影响。孕激素补充确实有重要的有益作用,但我们应该警惕在证据基础之外或之外进行治疗性给药。
卵子排出后,卵巢上会形成一个结构,称为黄体(CL)。它产生大量称为孕激素的激素。孕激素使子宫为怀孕做好准备,但如果没有怀孕,CL 在 12-14 天后消失,这会导致月经。如果怀孕了,那么妊娠激素(hCG)会使 CL 保持活力,其孕激素会在接下来的 6-8 周内支持妊娠,直到胎盘接管并使 CL 消失。这意味着如果 CL 不能正常工作,可能会出现怀孕或妊娠困难的问题。如果 CL 不能产生足够的孕激素,通常意味着卵子的生长或释放存在问题,治疗应集中在这些方面。在 IVF 周期中,正常激素被关闭,CL 在妊娠试验前不能产生足够的孕激素,此时需要额外的孕激素。然而,在反复性或威胁性流产中,没有证据表明 CL 工作不正常或孕激素水平低。但是,如果有反复流产史的女性在早期妊娠时出血,服用额外的孕激素是有益的。这可能是因为高剂量孕激素对子宫或免疫系统的影响。由于妊娠期间激素环境的变化可能对后代产生终身影响,因此我们必须谨慎,只有在确定需要时才给予额外的孕激素。