Wang Hui, Huang Jie, Yang Shuang, Zhang Xing-Fei, Yang Xiaoyan, Cui Chang, Zou Chan, Li Li-E, Zhang Min, Mao Miao-Fu, Zhou Xiang, Duan Kai-Ming, Wang Sai-Ying, Yang Guo-Ping
Center for Clinical Pharmacology, The Third Xiangya Hospital, Central South University, Changsha, 410013, Hunan, China.
Yichang Renfu Pharmaceutical Co., Ltd., Yichang, 443000, Hubei, China.
Neurol Ther. 2022 Jun;11(2):621-632. doi: 10.1007/s40120-022-00329-9. Epub 2022 Feb 7.
Buccal midazolam treatment is licensed in the European Union for prolonged acute convulsive seizures in children and adolescents, but the buccal pathway is often hampered by jaw clenching, hypersalivation, or uncontrolled swallowing. Midazolam formulations that are more secure, reliable, and faster for use are needed in the acute setting. Pharmacokinetics and comparative bioavailability of intranasally administered midazolam and two midazolam intravenous solutions administered buccally or intravenously in healthy adults were evaluated.
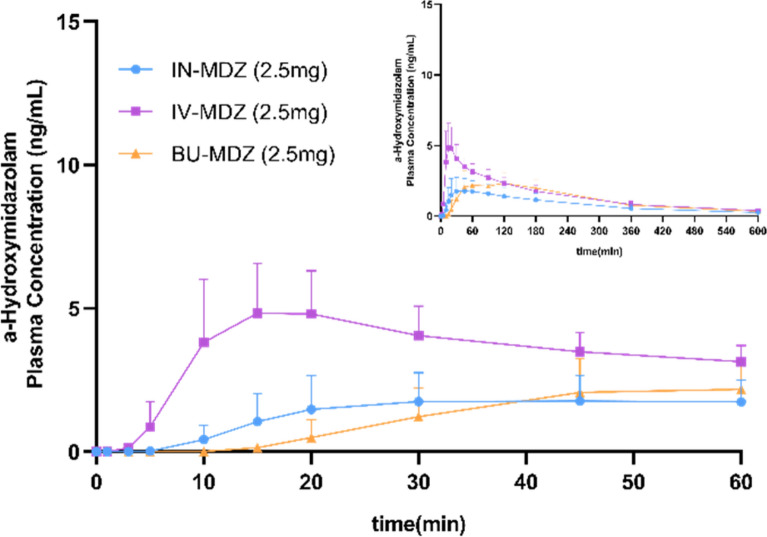
In this phase 1, open-label, randomized, single-dose, three-period, three-sequence crossover study, 12 healthy adults (19-41 years) were randomly assigned to receive 2.5 mg midazolam intranasally; 2.5 mg midazolam intravenously; 2.5 mg midazolam buccally. Blood samples were collected for 10 h post dose to determine pharmacokinetic profiles. Adverse events and vital signs were recorded.
Intranasal administration of 2.5 mg midazolam demonstrated a more rapid median time to C compared to buccal administration of midazolam (T, 12.6 min vs. 45 min; C, 38.33 ng/ml vs. 24.97 ng/ml). The antiepileptic effect of intranasal and buccal midazolam treatment lasted less than 4 h and generally did not differ from intravenously administered midazolam. No serious adverse events or deaths were reported, and no treatment-emergent adverse events led to study discontinuation.
Intranasal administration of midazolam may be a preferable alternative to the currently approve buccal midazolam treatment for prolonged acute convulsive seizures in children and adolescents.
This study is registered at the Chinese Clinical Trial [ http://www.chictr.org.cn ] (ChiCTR2000032595) on 3 May, 2020.
在欧盟,口服咪达唑仑被批准用于治疗儿童和青少年的持续性急性惊厥发作,但口服途径常常会受到牙关紧闭、唾液分泌过多或无法控制的吞咽的阻碍。在急性情况下,需要更安全、可靠且使用更快的咪达唑仑制剂。评估了健康成年人鼻内给予咪达唑仑以及两种口服或静脉注射的咪达唑仑静脉溶液的药代动力学和比较生物利用度。
在这项1期、开放标签、随机、单剂量、三周期、三序列交叉研究中,12名健康成年人(19 - 41岁)被随机分配接受2.5毫克鼻内咪达唑仑;2.5毫克静脉注射咪达唑仑;2.5毫克口服咪达唑仑。给药后10小时采集血样以确定药代动力学特征。记录不良事件和生命体征。
与口服咪达唑仑相比,鼻内给予2.5毫克咪达唑仑的中位达峰时间更快(T,12.6分钟对45分钟;C,38.33纳克/毫升对24.97纳克/毫升)。鼻内和口服咪达唑仑治疗的抗癫痫作用持续时间不到4小时,总体上与静脉注射咪达唑仑没有差异。未报告严重不良事件或死亡,也没有因治疗中出现的不良事件导致研究中断。
对于儿童和青少年的持续性急性惊厥发作,鼻内给予咪达唑仑可能是目前批准的口服咪达唑仑治疗的更好替代方案。
本研究于2020年5月3日在中国临床试验注册中心(http://www.chictr.org.cn)注册(ChiCTR2000032595)。