From the Department of Neurology (J.S.), Center for Cognitive Neurology, New York University Grossman School of Medicine, New York; The Framingham Study (J.S., A.S.B., J.K.S., A.O., H.J.A., S.S.); Department of Biostatistics (A.S.B., J.K.S., A.O.), Boston University School of Public Health; Department of Neurology (A.S.B., H.J.A., S.S.), Boston University School of Medicine, MA; Department of Neurology (C.S.D.), University of California Davis; and Glenn Biggs Institute for Alzheimer's and Neurodegenerative Diseases (M.M.G., S.S.), University of Texas Health Sciences Center, San Antonio.
Neurology. 2022 Mar 29;98(13):e1337-e1348. doi: 10.1212/WNL.0000000000200039. Epub 2022 Feb 7.
Loneliness is common, and its prevalence is rising. The relationship of loneliness with subsequent dementia and the early preclinical course of Alzheimer disease and related dementia (ADRD) remains unclear. Thus, the primary objective of this study was to determine the association of loneliness with 10-year all-cause dementia risk and early cognitive and neuroanatomic imaging markers of ADRD vulnerability.
This was a retrospective analysis of prospectively collected data from the population-based Framingham Study cohorts (September 9, 1948-December 31, 2018). Eligible participants had loneliness assessed and were dementia-free at baseline. Loneliness was recorded with the Center for Epidemiologic Studies Depression Scale, defined conservatively as feeling lonely ≥3 days in the past week. The main outcomes were incident dementia over a 10-year period, cognition, and MRI brain volumes and white matter injury.
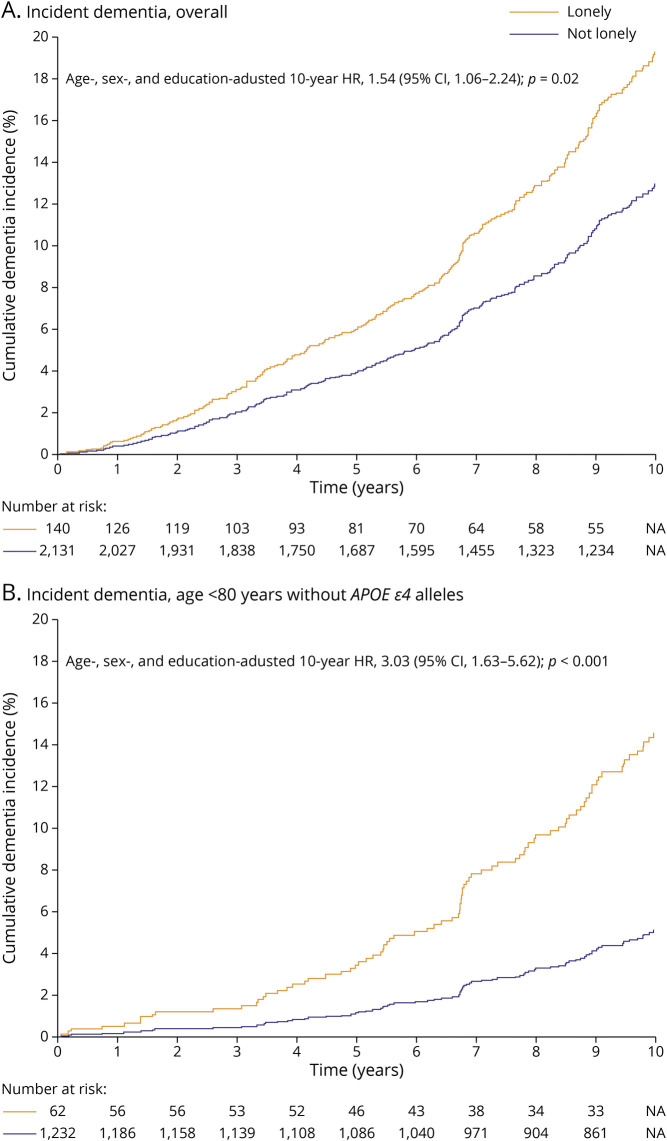
Of 2,308 participants (mean age 73 [SD 9] years, 56% women) who met eligibility in the dementia sample, 14% (329 of 2,308) developed dementia and 6% (144 of 2,308) were lonely. Lonely (versus not lonely) adults had higher 10-year dementia risk (age-, sex-, and education-adjusted hazard ratio 1.54, 95% CI 1.06-2.24). Lonely participants <80 years of age without ε4 alleles had a 3-fold greater risk (adjusted hazard ratio 3.03, 95% CI, 1.63-5.62). Among 1,875 persons without dementia who met eligibility in the cognition sample (mean age 62 [SD 9] years, 54% women), loneliness associated with poorer executive function, lower total cerebral volume, and greater white matter injury.
Over 10 years of close clinical dementia surveillance in this cohort study, loneliness was associated with increased dementia risk; this tripled in adults whose baseline risk would otherwise be relatively low on the basis of age and genetic risk, representing a majority of the US population. Loneliness was also associated with worse neurocognitive markers of ADRD vulnerability, suggesting an early pathogenic role. These findings may have important clinical and public health implications given observed loneliness trends.
This study provides Class I evidence that loneliness increases the 10-year risk of developing dementia.
孤独是常见的,而且其患病率正在上升。孤独与随后的痴呆症以及阿尔茨海默病和相关痴呆症(ADRD)的早期临床前病程之间的关系尚不清楚。因此,本研究的主要目的是确定孤独与 10 年全因痴呆风险以及 ADRD 易感性的早期认知和神经影像学标志物之间的关系。
这是一项对基于人群的弗雷明汉研究队列(1948 年 9 月 9 日至 2018 年 12 月 31 日)进行的前瞻性数据的回顾性分析。合格的参与者在基线时有孤独感评估且无痴呆症。孤独感通过流行病学研究中心抑郁量表记录,保守定义为过去一周内≥3 天感到孤独。主要结局是在 10 年内发生痴呆症,认知以及 MRI 脑容量和白质损伤。
在符合痴呆症样本入选标准的 2308 名参与者(平均年龄 73 [9]岁,56%为女性)中,有 14%(329 名/2308 名)发生痴呆症,有 6%(144 名/2308 名)为孤独者。孤独(与不孤独相比)成年人的 10 年痴呆风险更高(年龄、性别和教育调整后的风险比 1.54,95%CI 1.06-2.24)。没有 ε4 等位基因的年龄<80 岁的孤独参与者风险增加 3 倍(调整后的风险比 3.03,95%CI,1.63-5.62)。在认知样本中符合入选标准的 1875 名无痴呆症的人中(平均年龄 62 [9]岁,54%为女性),孤独与执行功能下降、总脑容量降低和白质损伤增加有关。
在这项队列研究中,经过 10 年的密切临床痴呆监测,孤独与痴呆风险增加相关;对于基线风险根据年龄和遗传风险相对较低的成年人,这一风险增加了三倍,这代表了美国人口的大多数。孤独也与 ADRD 易感性的神经认知标志物恶化有关,表明其具有早期发病作用。鉴于观察到的孤独趋势,这些发现可能具有重要的临床和公共卫生意义。
本研究提供了 I 级证据,表明孤独会增加 10 年发生痴呆症的风险。