Faculty of Business and Economics, University of Augsburg, Universitätsstraße 16, 86159, Augsburg, Germany.
Unit of Digitalization and Business Analytics, Universitätsklinikum Augsburg, Stenglinstraße 2, 86156, Augsburg, Germany.
Health Care Manag Sci. 2022 Jun;25(2):311-332. doi: 10.1007/s10729-021-09588-8. Epub 2022 Feb 9.
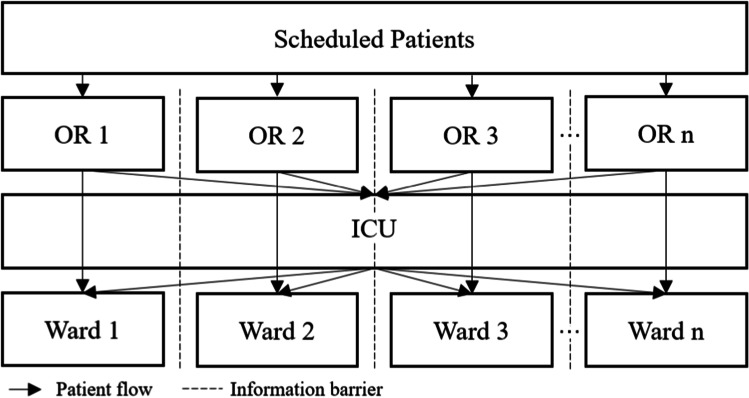
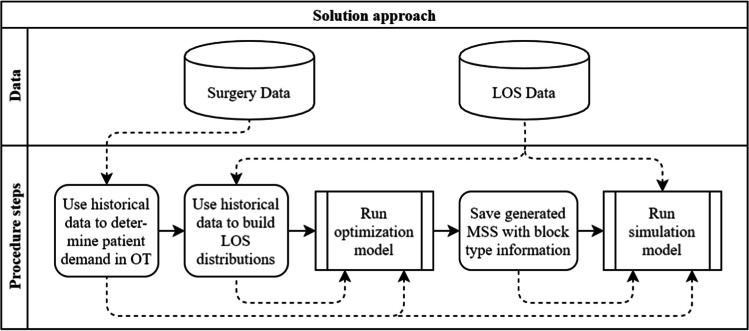
When scheduling surgeries in the operating theater, not only the resources within the operating theater have to be considered but also those in downstream units, e.g., the intensive care unit and regular bed wards of each medical specialty. We present an extension to the master surgery schedule, where the capacity for surgeries on ICU patients is controlled by introducing downstream-dependent block types - one for both ICU and ward patients and one where surgeries on ICU patients must not be performed. The goal is to provide better control over post-surgery patient flows through the hospital while preserving each medical specialty's autonomy over its operational surgery scheduling. We propose a mixed-integer program to determine the allocation of the new block types within either a given or a new master surgery schedule to minimize the maximum workload in downstream units. Using a simulation model supported by seven years of data from the University Hospital Augsburg, we show that the maximum workload in the intensive care unit can be reduced by up to 11.22% with our approach while maintaining the existing master surgery schedule. We also show that our approach can achieve up to 79.85% of the maximum workload reduction in the intensive care unit that would result from a fully centralized approach. We analyze various hospital setting instances to show the generalizability of our results. Furthermore, we provide insights and data analysis from the implementation of a quota system at the University Hospital Augsburg.
在安排手术室手术时,不仅要考虑手术室内部的资源,还要考虑下游科室的资源,例如重症监护病房和各医疗专业的常规床位病房。我们提出了一种主手术计划的扩展,其中通过引入下游相关的阻塞类型来控制 ICU 患者的手术能力——一种适用于 ICU 和病房患者,另一种则不允许对 ICU 患者进行手术。其目标是通过更好地控制手术后患者在医院内的流动,同时保留各医疗专业对其手术计划的自主运营,来提供更好的控制。我们提出了一个混合整数规划问题,以确定在给定或新的主手术计划中分配新的阻塞类型,从而将下游科室的最大工作量最小化。我们使用一个仿真模型,该模型基于奥格斯堡大学医院七年的数据,结果表明,通过我们的方法,重症监护病房的最大工作量可以减少多达 11.22%,同时保持现有的主手术计划。我们还表明,我们的方法可以实现重症监护病房最大工作量减少 79.85%,而这是完全集中式方法的结果。我们分析了各种医院环境实例,以展示我们的结果的普遍性。此外,我们还提供了奥格斯堡大学医院实施配额系统的见解和数据分析。