Department of Radiology, Albert Einstein College of Medicine and Montefiore Medical Center, Bronx, New York, United States.
Department of Applied Mathematics and Statistics, Stony Brook University, Stony Brook, New York, United States.
EBioMedicine. 2022 Feb;76:103821. doi: 10.1016/j.ebiom.2022.103821. Epub 2022 Feb 7.
Although acute cardiac injury (ACI) is a known COVID-19 complication, whether ACI acquired during COVID-19 recovers is unknown. This study investigated the incidence of persistent ACI and identified clinical predictors of ACI recovery in hospitalized patients with COVID-19 2.5 months post-discharge.
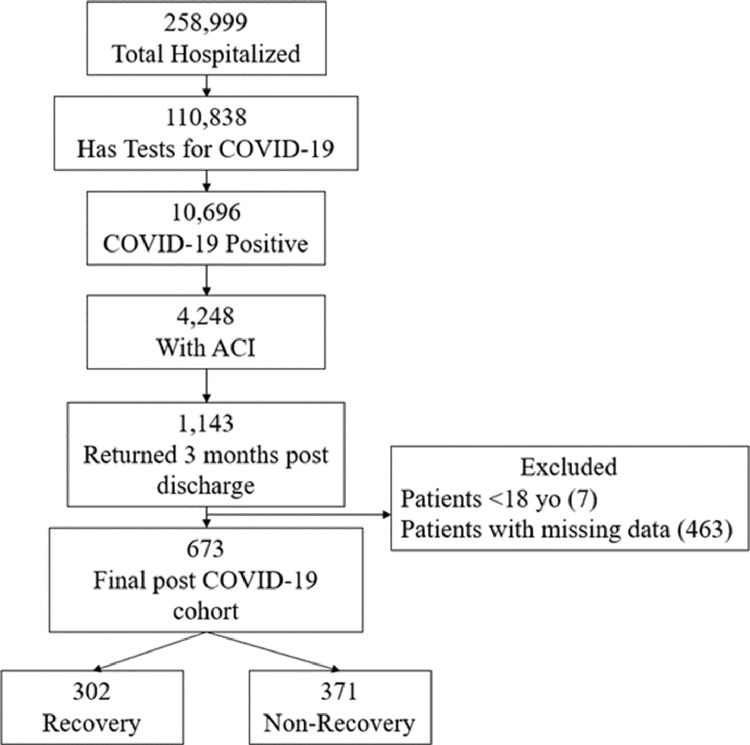
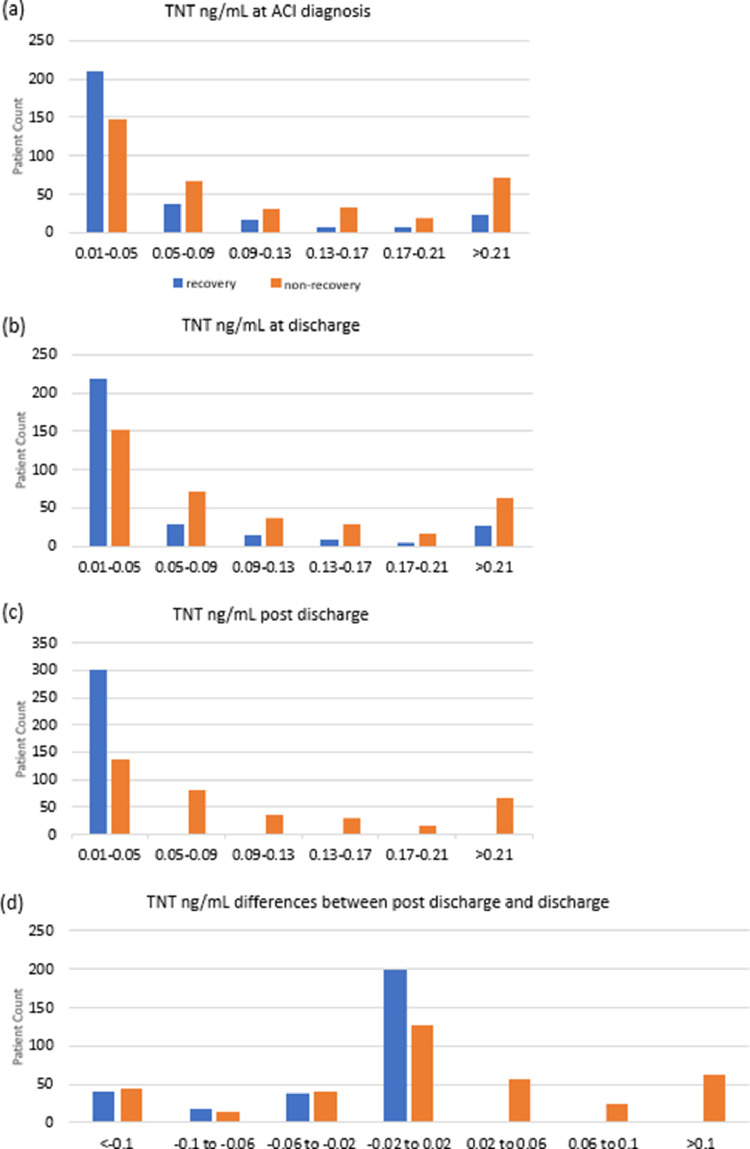
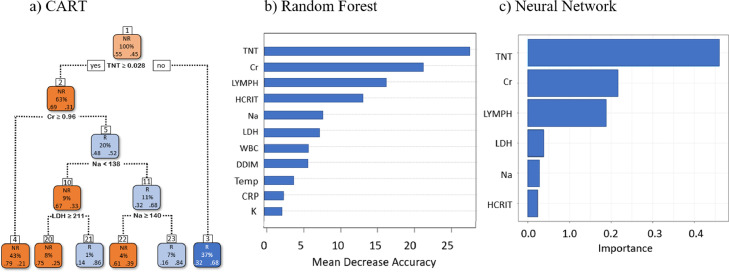
This retrospective study consisted of 10,696 hospitalized COVID-19 patients from March 11, 2020 to June 3, 2021. Demographics, comorbidities, and laboratory tests were collected at ACI onset, hospital discharge, and 2.5 months post-discharge. ACI was defined as serum troponin-T (TNT) level >99th-percentile upper reference limit (0.014ng/mL) during hospitalization, and recovery was defined as TNT below this threshold 2.5 months post-discharge. Four models were used to predict ACI recovery status.
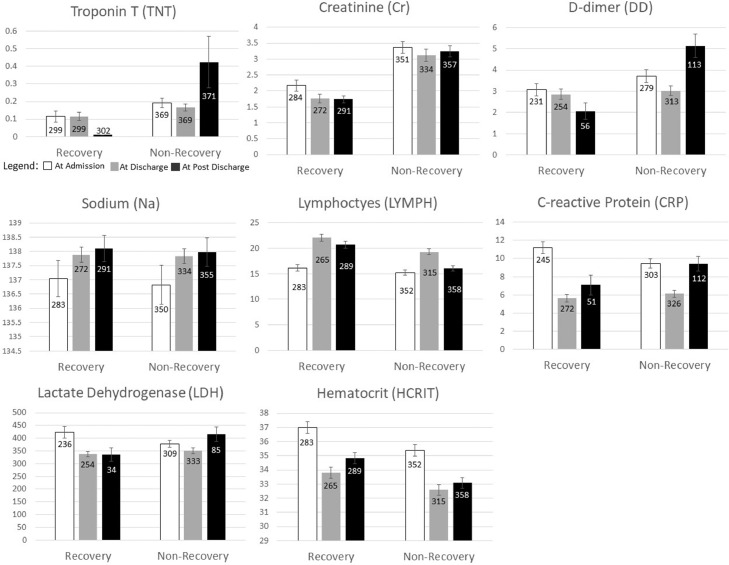
There were 4,248 (39.7%) COVID-19 patients with ACI, with most (93%) developed ACI on or within a day after admission. In-hospital mortality odds ratio of ACI patients was 4.45 [95%CI: 3.92, 5.05, p<0.001] compared to non-ACI patients. Of the 2,880 ACI survivors, 1,114 (38.7%) returned to our hospitals 2.5 months on average post-discharge, of which only 302 (44.9%) out of 673 patients recovered from ACI. There were no significant differences in demographics, race, ethnicity, major commodities, and length of hospital stay between groups. Prediction of ACI recovery post-discharge using the top predictors (troponin, creatinine, lymphocyte, sodium, lactate dehydrogenase, lymphocytes and hematocrit) at discharge yielded 63.73%-75.73% accuracy.
Persistent cardiac injury is common among COVID-19 survivors. Readily available patient data accurately predict ACI recovery post-discharge. Early identification of at-risk patients could help prevent long-term cardiovascular complications.
None.
虽然急性心脏损伤(ACI)是 COVID-19 的已知并发症,但 COVID-19 期间发生的 ACI 是否可以恢复尚不清楚。本研究旨在调查出院后 2.5 个月时 COVID-19 住院患者持续性 ACI 的发生率,并确定 ACI 恢复的临床预测因素。
本回顾性研究纳入了 2020 年 3 月 11 日至 2021 年 6 月 3 日期间的 10696 例 COVID-19 住院患者。在 ACI 发病时、出院时和出院后 2.5 个月收集人口统计学、合并症和实验室检查数据。ACI 定义为住院期间血清肌钙蛋白 T(TNT)水平>99 百分位参考上限(0.014ng/mL),恢复定义为出院后 2.5 个月时 TNT 低于该阈值。使用了 4 种模型来预测 ACI 恢复状态。
有 4248 例(39.7%)COVID-19 患者发生 ACI,其中大多数(93%)在入院当天或入院后一天内发生 ACI。与非 ACI 患者相比,ACI 患者的住院死亡率比值比为 4.45[95%CI:3.92,5.05,p<0.001]。在 2880 例 ACI 幸存者中,平均出院后 2.5 个月有 1114 例(38.7%)返回我院,其中仅 673 例患者中的 302 例(44.9%)从 ACI 中恢复。各组之间在人口统计学、种族、民族、主要商品和住院时间方面无显著差异。使用出院时的最佳预测因子(肌钙蛋白、肌酐、淋巴细胞、钠、乳酸脱氢酶、淋巴细胞和血细胞比容)对出院后 ACI 恢复情况进行预测,准确率为 63.73%-75.73%。
COVID-19 幸存者中持续性心脏损伤较为常见。现有患者数据可准确预测出院后 ACI 恢复情况。早期识别高危患者有助于预防长期心血管并发症。
无。