Singh Vinita, Gillespie Theresa W, Lane Olabisi, Spektor Boris, Zarrabi Ali John, Egan Katherine, Curseen Kimberly, Tsvetkova Maya, Beumer Jan H, Sniecinski Roman, Shteamer Jack W, Switchenko Jeffery, Harvey R Donald
Department of Anesthesiology, Emory University School of Medicine, Atlanta, Georgia, USA.
Department of Hematology and Medical Oncology, Emory University School of Medicine, Atlanta, Georgia, USA.
Pharmacotherapy. 2022 Apr;42(4):298-310. doi: 10.1002/phar.2669. Epub 2022 Feb 21.
The objective of our study was to determine safety and pharmacology (pharmacokinetics and preliminary efficacy) of intranasal (IN) ketamine for uncontrolled cancer-related pain.
Dose escalation clinical trial.
Outpatient.
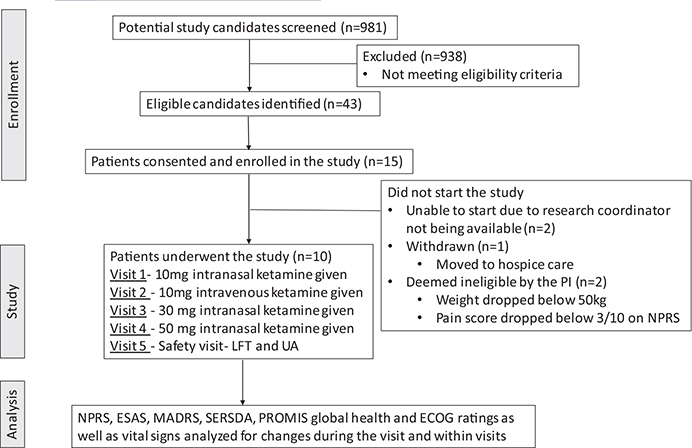
Ten adult patients with uncontrolled cancer-related pain.
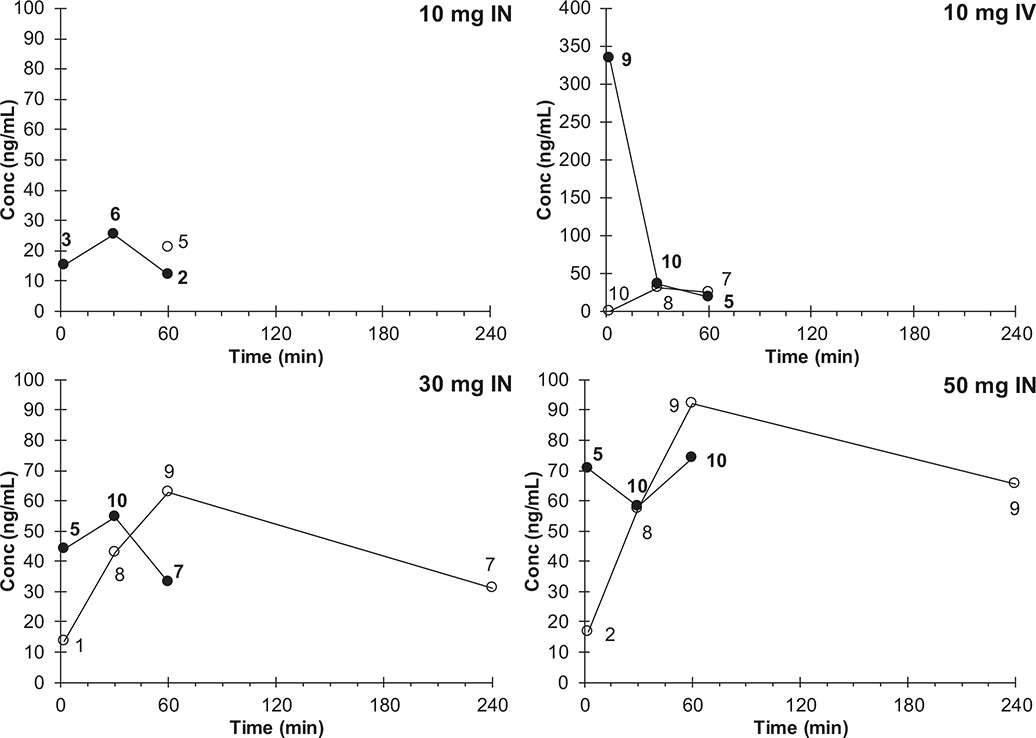
Each patient received escalating doses of ketamine over four visits, each 2-5 days apart: 10 mg IN at visit 1, 10 mg intravenous (IV) at visit 2, 30 mg IN at visit 3, and 50 mg IN at visit 4.
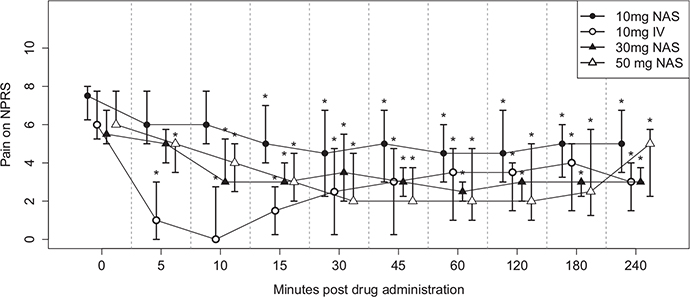
Pain was measured before and after drug administration for up to 4 h using the 11 point (0-10) Numerical Pain Rating Scale (NPRS).
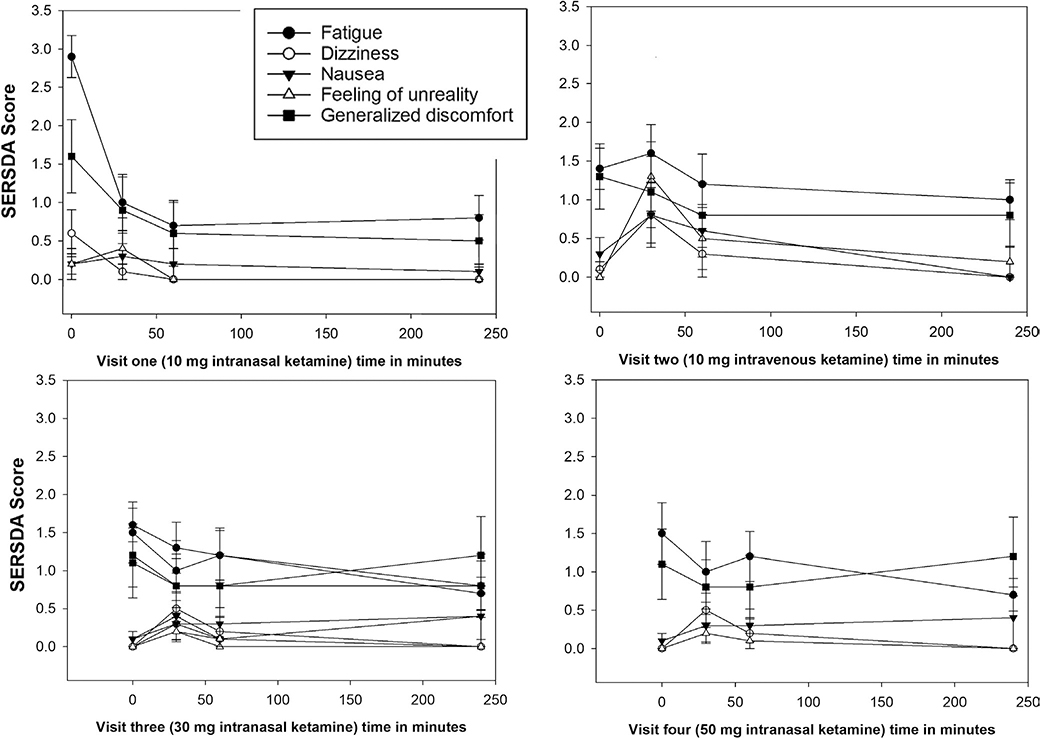
All subjects had advanced cancer, with intractable pain, despite being on moderate dosage of opioids. There was a statistically significant reduction in median NPRS by 1.5 (1-4), 3 (2-3), and 4 (3-5) points at 60 min after receiving the medication and remained decreased by 1.5 (1-2), 2 (1-2) and 1 (1-4) points at the end of the study visit (240 min) with the 10 mg, 30 mg and 50 mg IN dosage, respectively. The median percentage of maximal pain relief being 22.5 (16.6-71.5), 65.5 (40-100), and 69.25 (50-100) for 10 mg, 30 mg and 50 mg IN dosage, respectively and 100 (75-100) with 10 mg IV dose. All side effects (nausea and feeling of unreality) resolved by the end of each study visit. No severe adverse events occurred.
In this single-institution study, all dosages of IN ketamine administered in the study (10, 30, and 50 mg) provided significant pain relief for intractable cancer-related pain and were well tolerated. The 50 mg dose provided maximal pain relief without major side effects. Further study focused on repeated administration efficacy and safety for cancer-related pain is warranted.
我们研究的目的是确定鼻内给予氯胺酮治疗无法控制的癌症相关疼痛的安全性和药理学特性(药代动力学和初步疗效)。
剂量递增临床试验。
门诊。
10名患有无法控制的癌症相关疼痛的成年患者。
每位患者在四次就诊时接受递增剂量的氯胺酮,每次就诊间隔2 - 5天:第1次就诊时给予10mg鼻内用药,第2次就诊时给予10mg静脉注射,第3次就诊时给予30mg鼻内用药,第4次就诊时给予50mg鼻内用药。
使用11分制(0 - 10)数字疼痛评分量表(NPRS)在给药前和给药后长达4小时测量疼痛程度。
所有受试者均患有晚期癌症,尽管使用了中等剂量的阿片类药物,但仍有顽固性疼痛。用药后60分钟时,10mg、30mg和50mg鼻内用药剂量组的NPRS中位数分别显著降低1.5(1 - 4)、3(2 - 3)和4(3 - 5)分,在研究就诊结束时(240分钟)分别仍降低1.5(1 - 2)、2(1 - 2)和1(1 - 4)分。10mg、30mg和50mg鼻内用药剂量组最大疼痛缓解的中位数百分比分别为22.5(16.6 - 71.5)、65.5(40 - 100)和69.25(50 - 100),10mg静脉注射剂量组为100(75 - 100)。所有副作用(恶心和现实感异常)在每次研究就诊结束时均消失。未发生严重不良事件。
在这项单机构研究中,研究中给予的所有鼻内氯胺酮剂量(10mg、30mg和50mg)均为顽固性癌症相关疼痛提供了显著的疼痛缓解,且耐受性良好。50mg剂量提供了最大程度的疼痛缓解且无主要副作用。有必要进一步开展针对癌症相关疼痛重复给药疗效和安全性的研究。