Department of Public Health and Nursing, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology (NTNU), Trondheim, Norway.
Emergency Department, St. Olavs Hospital, Trondheim, Norway.
BMC Pediatr. 2023 Aug 18;23(1):405. doi: 10.1186/s12887-023-04203-x.
Children in acute pain often receive inadequate pain relief, partly from difficulties administering injectable analgesics. A rapid-acting, intranasal (IN) analgesic may be an alternative to other parenteral routes of administration. Our review compares the efficacy, safety, and acceptability of intranasal analgesia to intravenous (IV) and intramuscular (IM) administration; and to compare different intranasal agents.
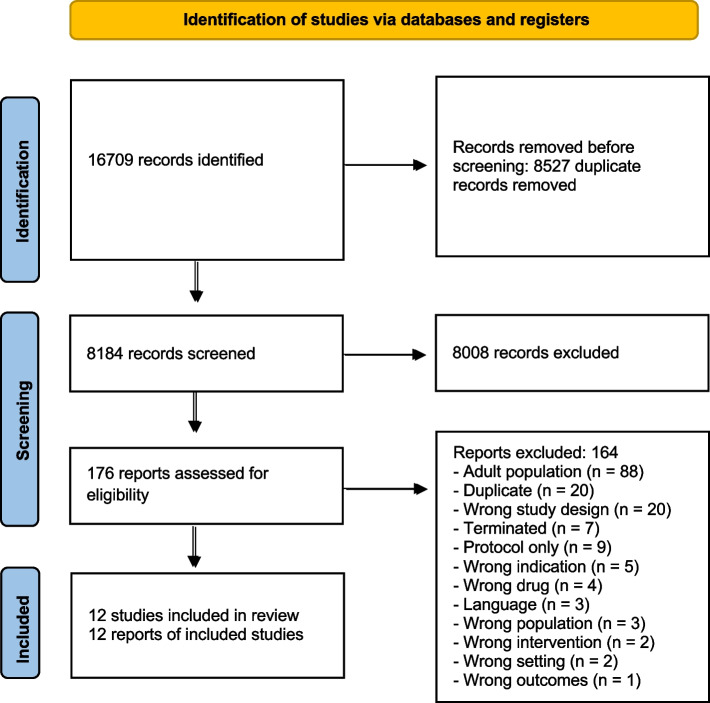
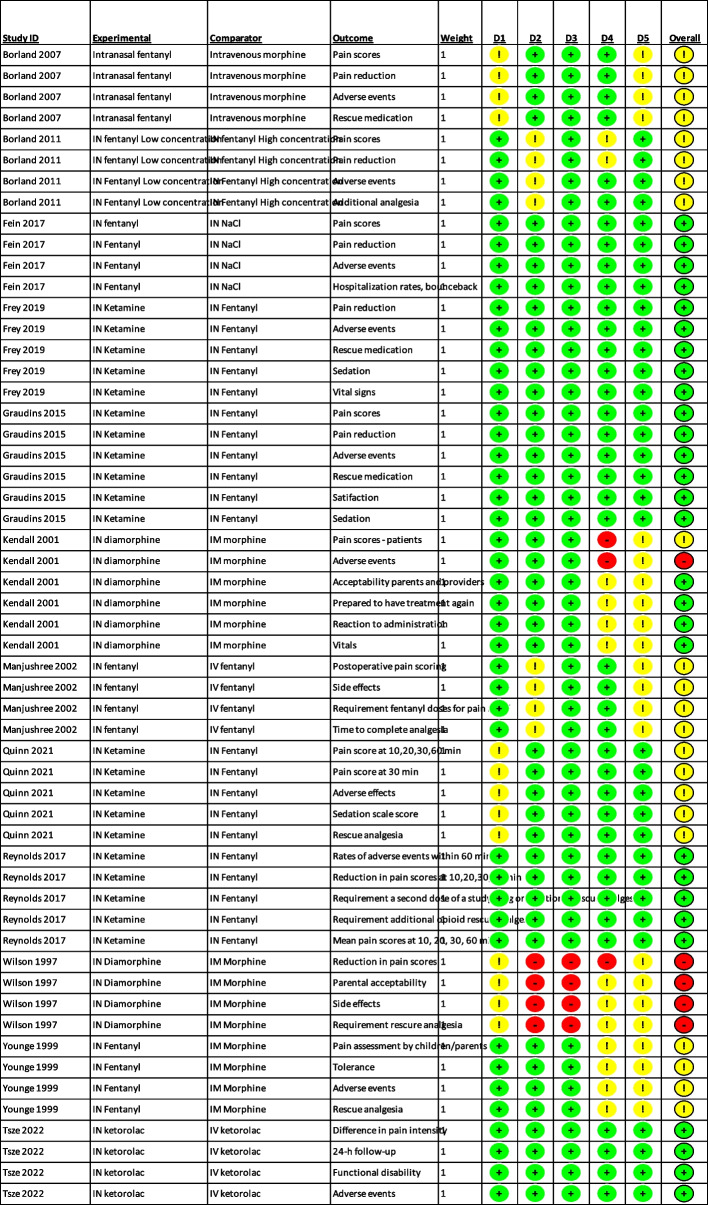
We searched Cochrane Library, MEDLINE/PubMed, Embase, Web of Knowledge, Clinicaltrials.gov, Controlled-trials.com/mrcr, Clinicaltrialsregister.eu, Apps.who.int/trialsearch. We also screened reference lists of included trials and relevant systematic reviews. Studies in English from any year were included. Two authors independently assessed all studies. We included randomised trials (RCTs) of children 0-16, with moderate to severe pain; comparing intranasal analgesia to intravenous or intramuscular analgesia, or to other intranasal agents. We excluded studies of procedural sedation or analgesia. We extracted study characteristics and outcome data and assessed risk of bias with the ROB 2.0-tool. We conducted meta-analysis and narrative review, evaluating the certainty of evidence using GRADE. Outcomes included pain reduction, adverse events, acceptability, rescue medication, ease of and time to administration.
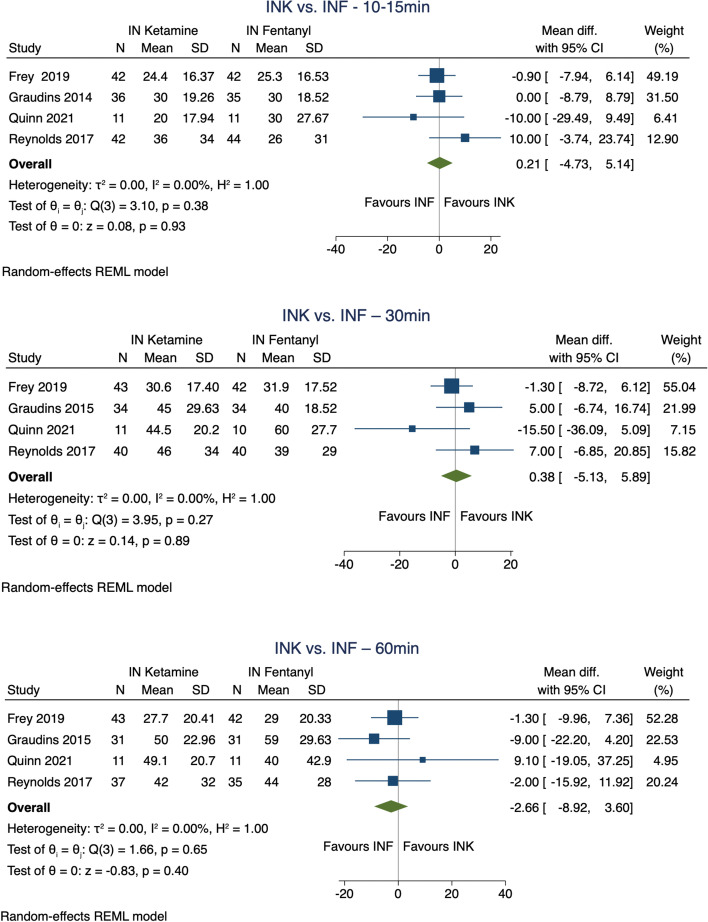
We included 12 RCTs with a total of 1163 children aged 3 to 20, most below 10 years old, with a variety of conditions. Our review shows that: - There may be little or no difference in pain relief (single dose IN vs IV fentanyl MD 4 mm, 95% CI -8 to 16 at 30 min by 100 mm VAS; multiple doses IN vs IV fentanyl MD 0, 95%CI -0.35 to 0.35 at 15 min by Hannallah score; single dose IN vs IV ketorolac MD 0.8, 95% CI -0.4 to 1.9 by Faces Pain Scale-Revised), adverse events (single dose IN vs IV fentanyl RR 3.09, 95% CI 0.34 to 28.28; multiple doses IN vs IV fentanyl RR 1.50, 95%CI 0.29 to 7.81); single dose IN vs IV ketorolac RR 0.716, 95% CI 0.23 to 2.26), or acceptability (single dose IN vs IV ketorolac RR 0.83, 95% CI 0.66 to 1.04) between intranasal and intravenous analgesia (low certainty evidence). - Intranasal diamorphine or fentanyl probably give similar pain relief to intramuscular morphine (narrative review), and are probably more acceptable (RR 1.60, 95% CI 1.42 to 1.81) and tolerated better (RR 0.061, 95% CI 0.03 to 0.13 for uncooperative/negative reaction) (moderate certainty); adverse events may be similar (narrative review) (low certainty). - Intranasal ketamine gives similar pain relief to intranasal fentanyl (SMD 0.05, 95% CI -0.20 to 0.29 at 30 min), while having a higher risk of light sedation (RR 1.74, 95% CI 1.30 to 2.35) and mild side effects (RR 2.16, 95% CI 1.72 to 2.71) (high certainty). Need for rescue analgesia is probably similar (RR 0.85, 95% CI 0.62 to 1.17) (moderate certainty), and acceptability may be similar (RR 1.15, 95% CI 0.89 to 1.48) (low certainty).
Our review suggests that intranasal analgesics are probably a good alternative to intramuscular analgesics in children with acute moderate to severe pain; and may be an alternative to intravenous administration. Intranasal ketamine gives similar pain relief to fentanyl, but causes more sedation, which should inform the choice of intranasal agent.
儿童急性疼痛常得不到充分缓解,部分原因是难以给予注射用镇痛剂。一种快速起效的鼻腔内(IN)镇痛剂可能是其他给药途径的替代方案。我们的综述比较了 IN 镇痛与静脉(IV)和肌肉内(IM)给药的疗效、安全性和可接受性;并比较了不同的鼻腔内制剂。
我们检索了 Cochrane 图书馆、MEDLINE/PubMed、Embase、Web of Knowledge、Clinicaltrials.gov、 Controlled-trials.com/mrcr、Clinicaltrialsregister.eu、Apps.who.int/trialsearch。我们还筛选了纳入试验和相关系统评价的参考文献列表。纳入了来自任何年份的英语研究。两名作者独立评估了所有研究。我们纳入了中度至重度疼痛的 0-16 岁儿童的随机对照试验(RCT);比较 IN 镇痛与 IV 或 IM 镇痛,或与其他 IN 制剂的比较。我们排除了程序性镇静或镇痛的研究。我们提取了研究特征和结局数据,并使用 ROB 2.0 工具评估了偏倚风险。我们进行了荟萃分析和叙述性综述,使用 GRADE 评估证据的确定性。结局包括疼痛缓解、不良事件、可接受性、解救药物、给药的难易程度和时间。
我们纳入了 12 项 RCT,共纳入了 1163 名年龄在 3 至 20 岁的儿童,大多数年龄在 10 岁以下,患有各种疾病。我们的综述表明:-IN 与 IV 芬太尼相比,单次剂量 IN 对疼痛缓解可能没有或仅有轻微差异(30 分钟时 100mm VAS 疼痛评分的 4mm,MD -8 至 16;15 分钟时 Hannallah 评分的 MD 0.35 至 0.35);IN 与 IV 酮洛酸相比,多次剂量 IN 对疼痛缓解可能没有或仅有轻微差异(30 分钟时 Faces Pain Scale-Revised 疼痛评分的 MD 0.8,MD -0.4 至 1.9),不良事件(单次剂量 IN 与 IV 芬太尼的 RR 3.09,95%CI 0.34 至 28.28;多次剂量 IN 与 IV 芬太尼的 RR 1.50,95%CI 0.29 至 7.81);单次剂量 IN 与 IV 酮洛酸的 RR 0.716,95%CI 0.23 至 2.26),或可接受性(单次剂量 IN 与 IV 酮洛酸的 RR 0.83,95%CI 0.66 至 1.04),IN 与 IV 镇痛之间可能没有差异(低确定性证据)。-IN 二氢吗啡酮或芬太尼可能与 IM 吗啡产生相似的疼痛缓解效果(叙述性综述),并且可能更易被接受(RR 1.60,95%CI 1.42 至 1.81)和耐受性更好(RR 0.061,95%CI 0.03 至 0.13 用于不合作/不良反应)(中度确定性);不良事件可能相似(叙述性综述)(低确定性)。-IN 氯胺酮与 IN 芬太尼相比可能具有相似的镇痛效果(30 分钟时的 SMD 0.05,95%CI -0.20 至 0.29),而镇静作用较轻(RR 1.74,95%CI 1.30 至 2.35)和轻度副作用(RR 2.16,95%CI 1.72 至 2.71)(高确定性)。需要解救镇痛的可能性可能相似(RR 0.85,95%CI 0.62 至 1.17)(中度确定性),可接受性可能相似(RR 1.15,95%CI 0.89 至 1.48)(低确定性)。
我们的综述表明,在患有急性中重度疼痛的儿童中,IN 镇痛药可能是 IM 镇痛药的良好替代品;并且可能是 IV 给药的替代方案。IN 氯胺酮与芬太尼相比可能具有相似的镇痛效果,但会引起更多的镇静作用,这应告知 IN 制剂的选择。