Quach Duc Trong, Aoki Rika, Iga Akiko, Le Quang Dinh, Kawamura Toru, Yamashita Ken, Tanaka Shinji, Yoshihara Masaharu, Hiyama Toru
Department of Internal Medicine, University of Medicine and Pharmacy at Hochiminh City, Ho Chi Minh, Vietnam.
Department of Gastroenterology, Nhan Dan Gia Dinh Hospital, Ho Chi Minh, Vietnam.
Front Med (Lausanne). 2022 Jan 28;8:830730. doi: 10.3389/fmed.2021.830730. eCollection 2021.
To assess the time trend of diagnostic accuracy of pre- and post-eradication status and interobserver agreement of gastric atrophy grading.
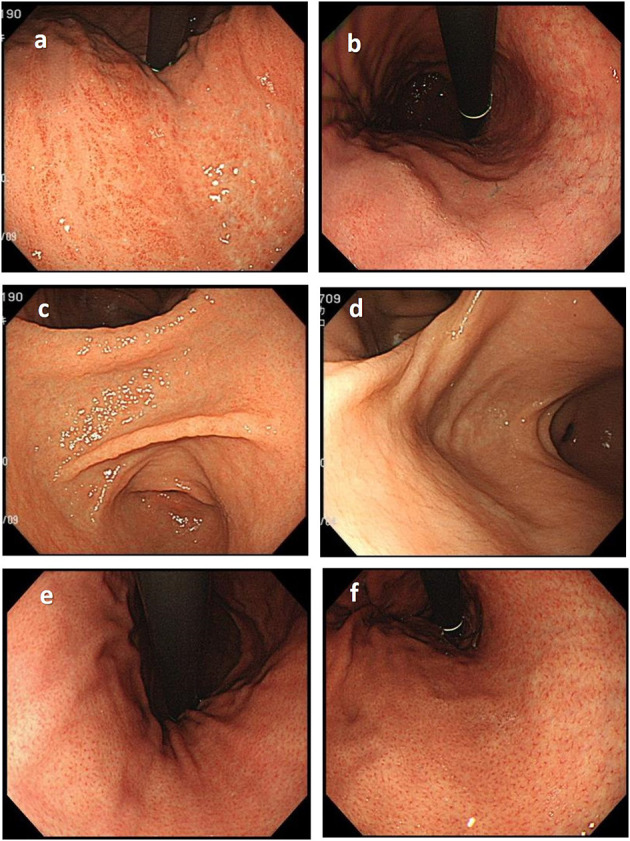
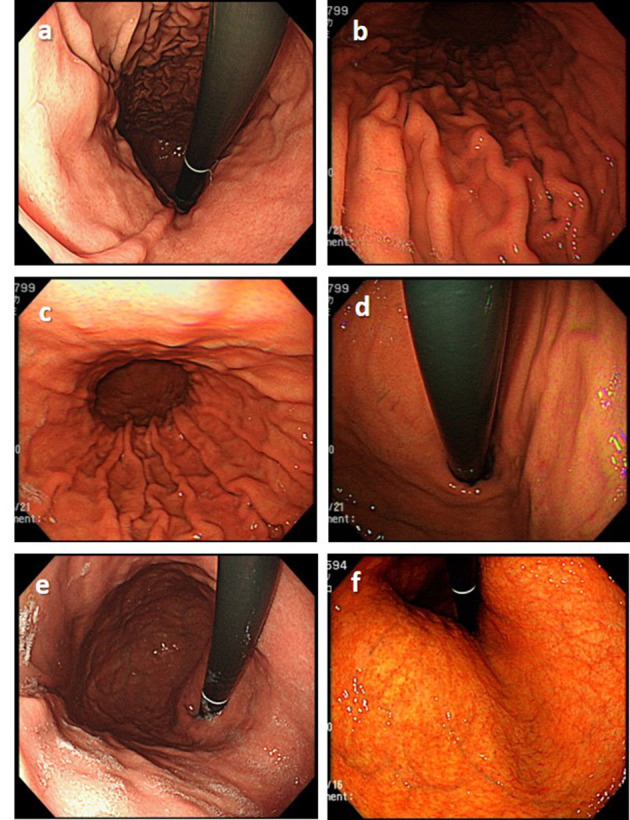
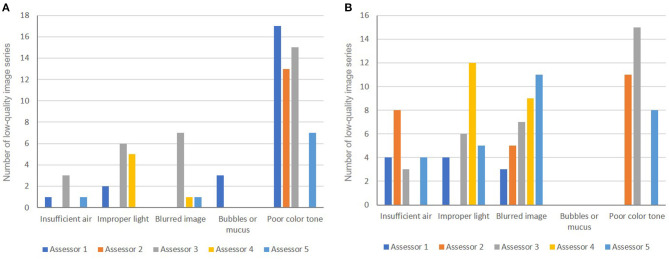
A series 100 of conventional endoscopic image sets taken from subjects undergoing gastric cancer screening at a polyclinic were evaluated by 5 experienced assessors. Each assessor independently examined endoscopic findings according to the Kyoto classification and then determined the status (never, current, or past infected). Gastric atrophy was assessed according to the Kimura-Takemoto classification and classified into 3 grades (none/mild, moderate, or severe). The image series that ≥3 assessors considered to have good quality were arbitrarily defined as high-quality image (HQI) series, and the rest were defined as low-quality image (LQI) series.
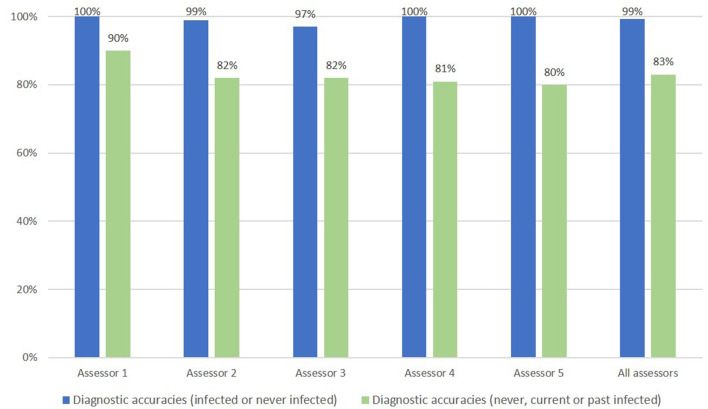
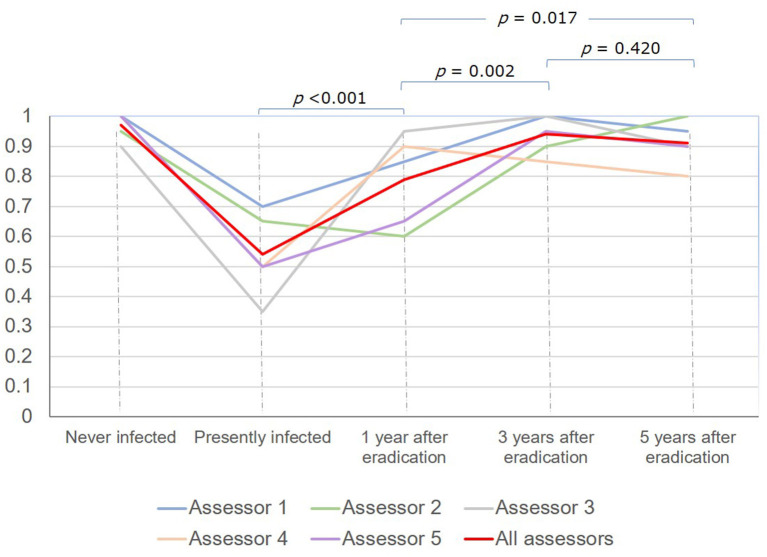
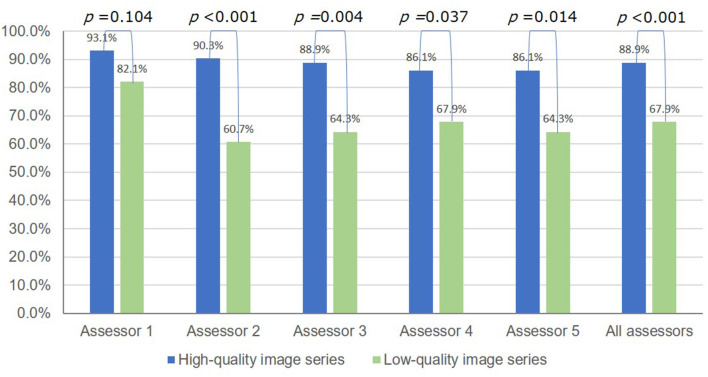
The overall diagnostic accuracy of status was 83.0%. It was lowest in subjects with current infection (54%), gradually increased at 1 year (79%, < 0.001) and 3 years (94.0%, = 0.002), but then did not significantly change at 5 years (91.0%, = 0.420) after eradication. The rate of LQI series was 28%. The overall diagnostic accuracy of status dropped from 88.9% to 67.9% ( < 0.001), and the mean kappa value on gastric atrophy grading dropped from 0.730 to 0.580 ( = 0.002) in the HQI and LQI series, respectively.
Diagnostic accuracy of status increased over time after eradication. LQI series badly affected the diagnostic accuracy of status and the level of agreement when grading gastric atrophy.
评估根除前后状态诊断准确性的时间趋势以及胃萎缩分级的观察者间一致性。
5名经验丰富的评估者对从一家综合诊所接受胃癌筛查的受试者中获取的100套传统内镜图像集进行评估。每位评估者根据京都分类法独立检查内镜检查结果,然后确定状态(从未感染、当前感染或既往感染)。根据木村 - 竹本分类法评估胃萎缩情况,并分为3级(无/轻度、中度或重度)。将≥3名评估者认为质量良好的图像系列任意定义为高质量图像(HQI)系列,其余的定义为低质量图像(LQI)系列。
状态的总体诊断准确性为83.0%。在当前感染的受试者中最低(54%),根除后1年(79%,P<0.001)和3年(94.0%,P = 0.002)时逐渐升高,但在5年时(91.0%,P = 0.420)无显著变化。LQI系列的比例为28%。在HQI和LQI系列中,状态的总体诊断准确性分别从88.9%降至67.9%(P<0.001),胃萎缩分级的平均kappa值分别从0.730降至0.580(P = 0.002)。
根除后状态的诊断准确性随时间增加。LQI系列严重影响状态的诊断准确性以及胃萎缩分级时的一致性水平。