Schwarze Julia Katharina, Garaud Soizic, Jansen Yanina J L, Awada Gil, Vandersleyen Valérie, Tijtgat Jens, de Wind Alexandre, Kristanto Paulus, Seremet Teofila, Willard-Gallo Karen, Neyns Bart
Department of Medical Oncology, Vrije Universiteit Brussel (VUB)/Universitair Ziekenhuis Brussel (UZ Brussel), Laarbeeklaan 101, 1090 Brussels, Belgium.
Molecular Immunology Unit, Institut Jules Bordet, Université Libre de Bruxelles, 1000 Brussels, Belgium.
Cancers (Basel). 2022 Jan 28;14(3):682. doi: 10.3390/cancers14030682.
Optimal dosing and duration of adjuvant treatment with PD-1 and CTLA-4 immune checkpoint inhibitors have not been established. Prior to their regulatory approval we investigated a low-dose regimen of nivolumab with or without ipilimumab in a sequential dual-cohort phase II clinical trial.
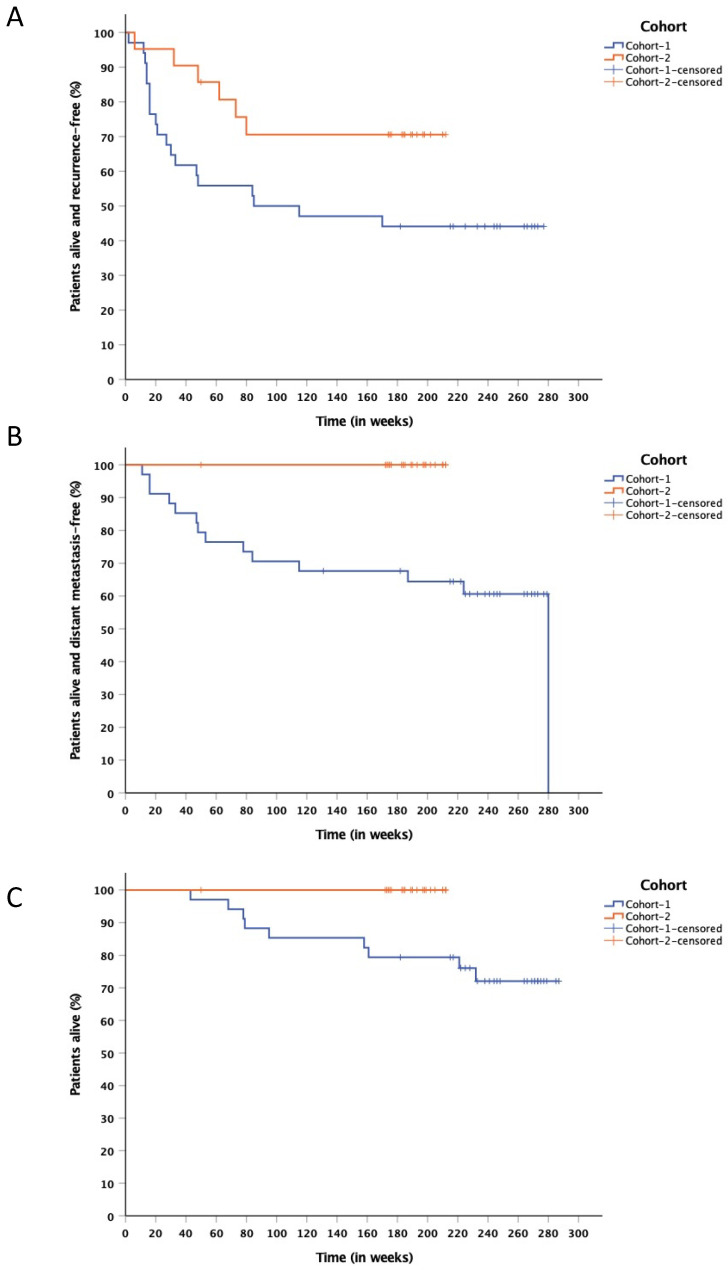
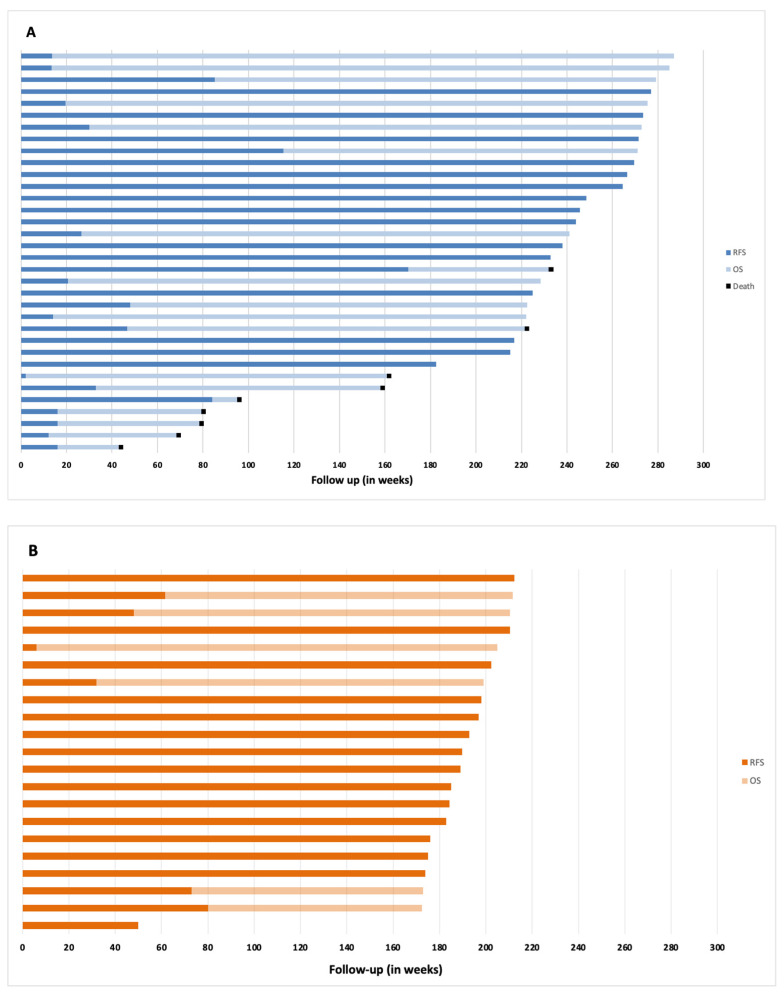
Following the complete resection of melanoma metastases, patients were treated with a single fixed dose of ipilimumab (50 mg) plus 4 bi-weekly fixed doses of nivolumab (10 mg) (cohort-1), or nivolumab for 1 year (10 mg fixed dose, Q2w x9, followed by Q8w x4) (cohort-2). Twelve-months relapse-free survival (RFS) served as the primary endpoint.
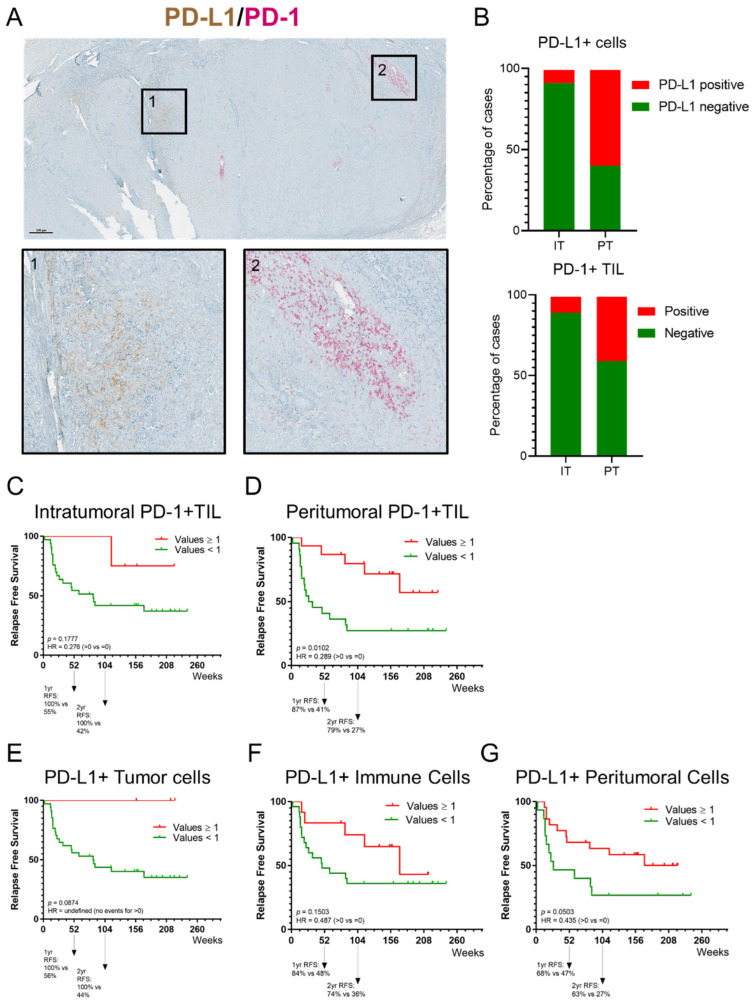
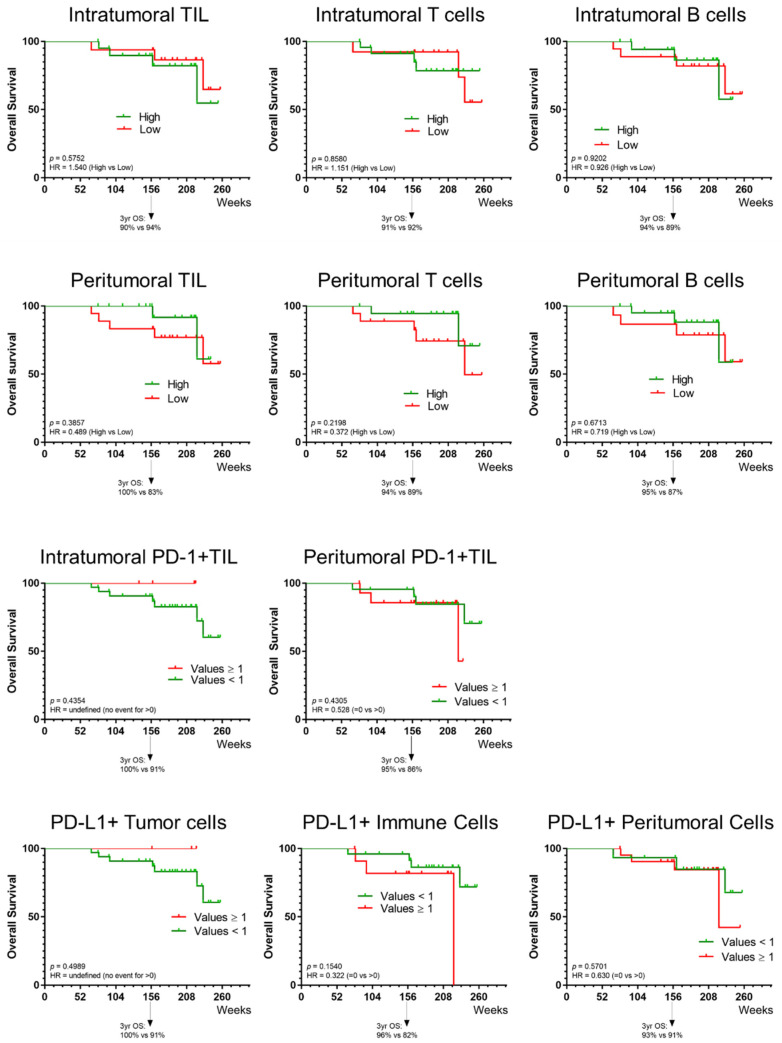
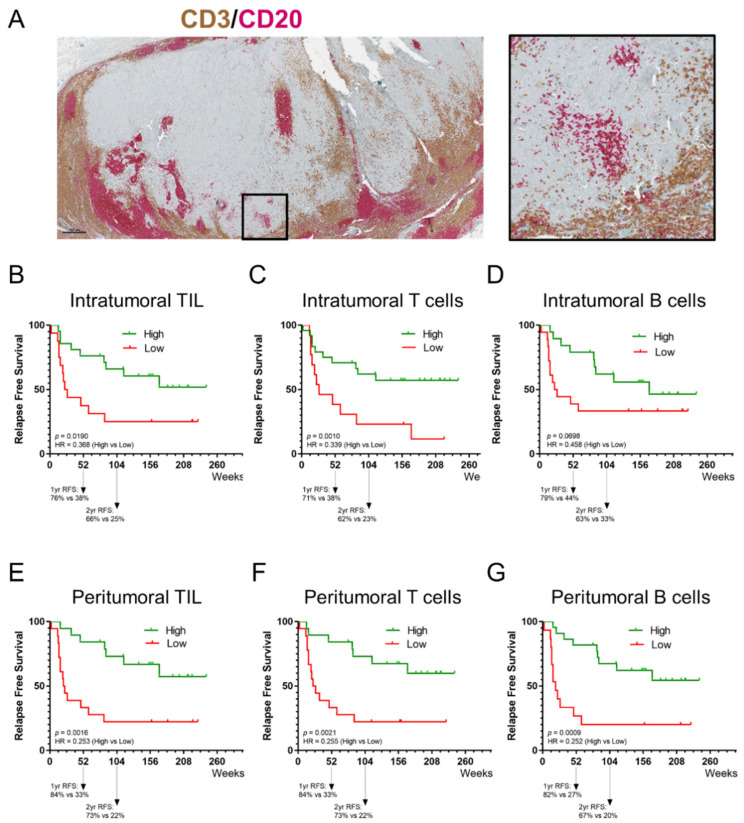
After a median follow-up of 235 weeks for cohort-1 (34 patients), and 190 weeks for cohort-2 (21 patients), the 12-months RFS-rate was, respectively, 55.9% (95% CI, 39-72), and 85.7% (95% CI, 70-100). Treatment-related adverse events occurred in 27 (79%), and 18 (86%) patients, with 3 (9%), and 1 (5%) grade 3 adverse events in cohort-1 and -2, respectively. Immunohistochemical quantification of intra- and peritumoral CD3 T cells and CD20 B cells, but not PD-1/PD-L1 staining, correlated significantly with RFS.
One year of adjuvant low-dose nivolumab could be an effective and economically advantageous alternative for standard dosing, at the condition of further confirmation in a larger patient cohort. A shorter low-dose nivolumab plus ipilimumab regimen seems inferior and less tolerable.
PD - 1和CTLA - 4免疫检查点抑制剂辅助治疗的最佳剂量和疗程尚未确定。在其获得监管批准之前,我们在一项序贯双队列II期临床试验中研究了纳武单抗联合或不联合伊匹单抗的低剂量方案。
黑色素瘤转移灶完全切除后,患者接受单次固定剂量的伊匹单抗(50mg)加4次每两周一次的固定剂量纳武单抗(10mg)(队列1),或接受纳武单抗治疗1年(固定剂量10mg,每2周一次,共9次,随后每8周一次,共4次)(队列2)。12个月无复发生存期(RFS)作为主要终点。
队列1(34例患者)中位随访235周,队列2(21例患者)中位随访190周,12个月RFS率分别为55.9%(95%CI,39 - 72)和85.7%(95%CI,70 - 100)。队列1和队列2分别有27例(79%)和18例(86%)患者发生治疗相关不良事件,3级不良事件分别有3例(9%)和1例(5%)。瘤内和瘤周CD3 T细胞及CD20 B细胞的免疫组化定量分析与RFS显著相关,而PD - 1/PD - L1染色则不然。
在更大患者队列中进一步证实的情况下,辅助低剂量纳武单抗治疗1年可能是标准剂量治疗的一种有效且经济上有利的替代方案。较短疗程的低剂量纳武单抗加伊匹单抗方案似乎疗效较差且耐受性较低。