Eleftheriadou Aikaterini, Francis Abraham, Wilcox Mark, Jayaprakasan Kanna
School of Medicine, University of Nottingham, Nottingham NG7 2RD, UK.
CARE Fertility, Nottingham NG8 6PZ, UK.
J Clin Med. 2022 Jan 29;11(3):737. doi: 10.3390/jcm11030737.
Various factors, including treatment protocols, can influence the outcomes of frozen embryo transfers (FETs). The study objectives were to compare different endometrial preparation protocols of FET cycles and to evaluate the factors, including the endometrial thickness (ET), that affect outcomes.
This observational cohort study involved 5037 women undergoing FETs at eight tertiary clinics in the UK between January 2016 and March 2019. The endometrial preparation protocols used were natural cycle (NC-FETs), artificial hormone support cycle with oestradiol valerate but without pituitary downregulation (AC-FETs) and artificial hormone support cycle with agonist downregulation (ACDR-FETs).
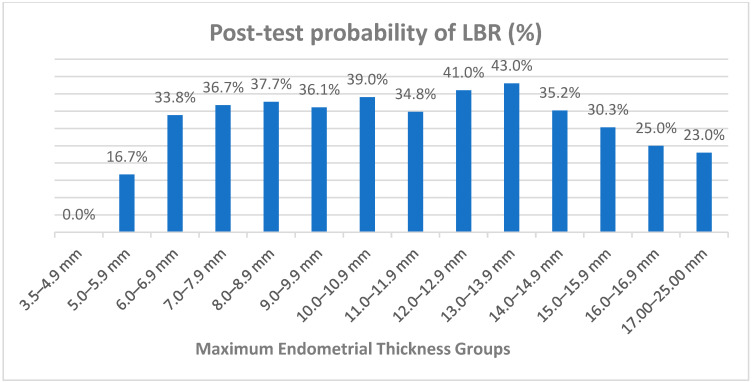
The mean (±SD) ages across NC-FET, AC-FET and ACDR-FET groups were 36.5 (±4.2), 35.9 (±5.0) and 36.4(±4.9) years, respectively. LBRs were comparable (40.7%, 175/430; 36.8%, 986/2658; and 36.7%, 716/1949, respectively) across the three groups. Clinical pregnancy, implantation, multiple pregnancies, miscarriage and ectopic pregnancy rates were also similar. In the regression analysis of variables including age, duration of infertility, number of embryos transferred, protocol type and endometrial thickness, age was the only significant predictor of LBRs, although its predictive ability was poor (AUC: 0.55). With the overall LBR of the study population being 37.1%, the post-test probability of a live birth at an ET of <5 mm was 0%, and at 5-5.9, 6-6.9, 7-7.9 and 8-8.9 mm, the probabilities were 16.7%, 33.8%, 36.7% and 37.7%, respectively. The LBR remained above 35% up to the 14-14.9 mm range and then declined gradually to 23% for the 17-25 mm range.
The FET outcomes were similar for the three protocols used for endometrial preparation. The protocol type and endometrial thickness were not predictive of FET outcomes; age was the only predictive variable, despite its low predictive ability.
包括治疗方案在内的多种因素会影响冷冻胚胎移植(FET)的结果。本研究的目的是比较FET周期中不同的子宫内膜准备方案,并评估影响结果的因素,包括子宫内膜厚度(ET)。
这项观察性队列研究纳入了2016年1月至2019年3月期间在英国八家三级诊所接受FET的5037名女性。所采用的子宫内膜准备方案为自然周期(NC-FET)、使用戊酸雌二醇但未进行垂体降调节的人工激素支持周期(AC-FET)以及使用激动剂降调节的人工激素支持周期(ACDR-FET)。
NC-FET组、AC-FET组和ACDR-FET组的平均(±标准差)年龄分别为36.5(±4.2)岁、35.9(±5.0)岁和36.4(±4.9)岁。三组的活产率相当(分别为40.7%,175/430;36.8%,986/2658;和36.7%,716/1949)。临床妊娠率、着床率、多胎妊娠率、流产率和异位妊娠率也相似。在对年龄、不孕持续时间、移植胚胎数量、方案类型和子宫内膜厚度等变量进行的回归分析中,年龄是活产率的唯一显著预测因素,尽管其预测能力较差(AUC:0.55)。研究人群的总体活产率为37.1%,子宫内膜厚度<5mm时活产的检验后概率为0%,在5-5.9mm、6-6.9mm、7-7.9mm和8-8.9mm时,概率分别为16.7%、33.8%、36.7%和37.7%。在14-14.9mm范围内,活产率保持在35%以上,然后在17-25mm范围内逐渐下降至23%。
用于子宫内膜准备的三种方案的FET结果相似。方案类型和子宫内膜厚度不能预测FET结果;年龄是唯一的预测变量,尽管其预测能力较低。