Asi Yara M, Bebasari Priliantina, Hardy Emily, Lokot Michelle, Meagher Kristen, Ogbe Emilomo, Parray Ateeb Ahmad, Sharma Vandana, Standley Claire J, Vahedi Luissa
School of Global Health Management and Informatics, University of Central Florida, Orlando, FL, USA.
Gender Specialist and Consultant, Jakarta, Indonesia.
Confl Health. 2022 Feb 14;16(1):4. doi: 10.1186/s13031-022-00435-3.
The COVID-19 pandemic has necessitated rapid development of preparedness and response plans to quell transmission and prevent illness across the world. Increasingly, there is an appreciation of the need to consider equity issues in the development and implementation of these plans, not least with respect to gender, given the demonstrated differences in the impacts both of the disease and of control measures on men, women, and non-binary individuals. Humanitarian crises, and particularly those resulting from conflict or violence, exacerbate pre-existing gender inequality and discrimination. To this end, there is a particularly urgent need to assess the extent to which COVID-19 response plans, as developed for conflict-affected states and forcibly displaced populations, are gender responsive.
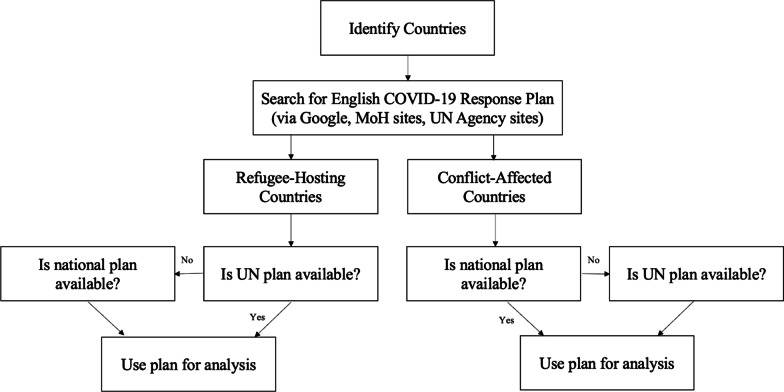
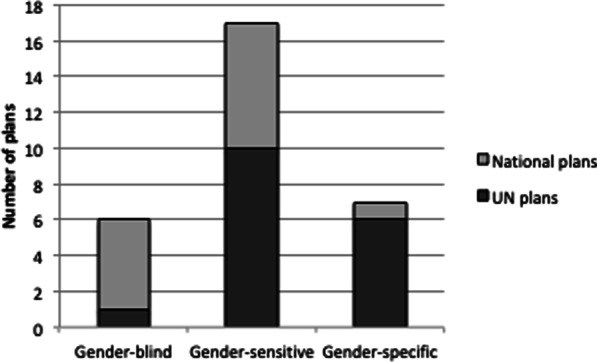
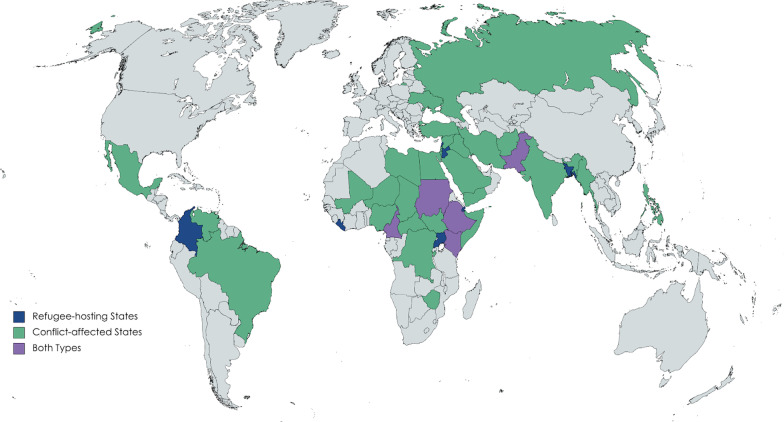
Using a multi-step selection process, we identified and analyzed 30 plans from states affected by conflict and those hosting forcibly displaced refugees and utilized an adapted version of the World Health Organization's Gender Responsive Assessment Scale (WHO-GRAS) to determine whether existing COVID-19 response plans were gender-negative, gender-blind, gender-sensitive, or gender-transformative.
We find that although few plans were gender-blind and none were gender-negative, no plans were gender-transformative. Most gender-sensitive plans only discuss issues specifically related to women (such as gender-based violence and reproductive health) rather than mainstream gender considerations throughout all sectors of policy planning.
Despite overwhelming evidence about the importance of intentionally embedding gender considerations into the COVID-19 planning and response, none of the plans reviewed in this study were classified as 'gender transformative.' We use these results to make specific recommendations for how infectious disease control efforts, for COVID-19 and beyond, can better integrate gender considerations in humanitarian settings, and particularly those affected by violence or conflict.
新冠疫情促使全球迅速制定防范和应对计划,以遏制病毒传播并预防疾病。人们越来越认识到,在制定和实施这些计划时需要考虑公平问题,尤其是性别方面的公平,因为已有证据表明,该疾病及其控制措施对男性、女性和非二元性别人群的影响存在差异。人道主义危机,尤其是由冲突或暴力引发的危机,会加剧原有的性别不平等和歧视。为此,特别迫切需要评估为受冲突影响国家和被迫流离失所人口制定的新冠应对计划在多大程度上对性别问题有响应。
我们通过多步骤筛选过程,识别并分析了来自受冲突影响国家以及收容被迫流离失所难民的国家的30份计划,并使用世界卫生组织性别响应评估量表(WHO-GRAS)的改编版来确定现有的新冠应对计划是性别消极型、性别盲视型、性别敏感型还是性别变革型。
我们发现,虽然很少有计划是性别盲视型的,也没有性别消极型的计划,但没有一个计划是性别变革型的。大多数性别敏感型计划只讨论与女性具体相关的问题(如基于性别的暴力和生殖健康),而不是在政策规划的所有部门中纳入主流性别考量。
尽管有大量证据表明在新冠规划和应对中有意纳入性别考量很重要,但本研究中审查的计划没有一个被归类为“性别变革型”。我们利用这些结果就如何在人道主义环境中,特别是在受暴力或冲突影响的环境中,让新冠及其他传染病防控工作更好地纳入性别考量提出具体建议。