Hepato-Gastroenterology and Digestive Oncology Department, University and Centre Hospitalier Univestitaire (CHU) Liège, Liège, Belgium.
Ferring International Center SA, Saint-Prex, Switzerland
BMJ Open Gastroenterol. 2022 Feb;9(1). doi: 10.1136/bmjgast-2021-000853.
5-aminosalicylate (mesalazine; 5-ASA) is an established first-line treatment for mild-to-moderate ulcerative colitis (UC). This study aimed to model the benefits of optimising 5-ASA therapy.
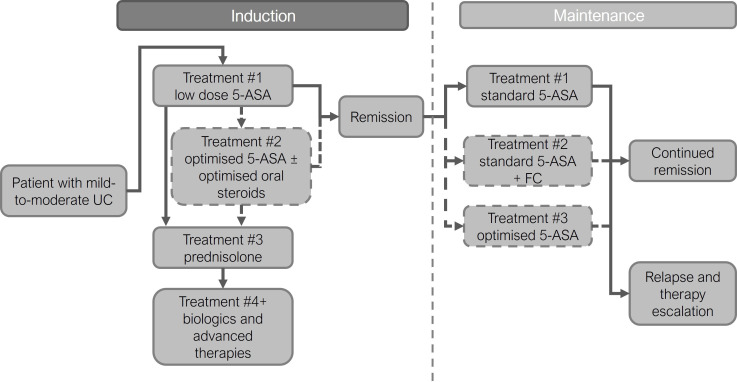
A decision tree model followed 10 000 newly diagnosed patients with mild-to-moderately active UC through induction and 1 year of maintenance treatment. Optimised treatment (maximising dose of 5-ASA and use of combined oral and rectal therapy before treatment escalation) was compared with standard treatment (standard doses of 5-ASA without optimisation). Modelled data were derived from published meta-analyses. The primary outcomes were patient numbers achieving and maintaining remission, with an analysis of treatment costs for each strategy conducted as a secondary outcome (using UK reference costs).
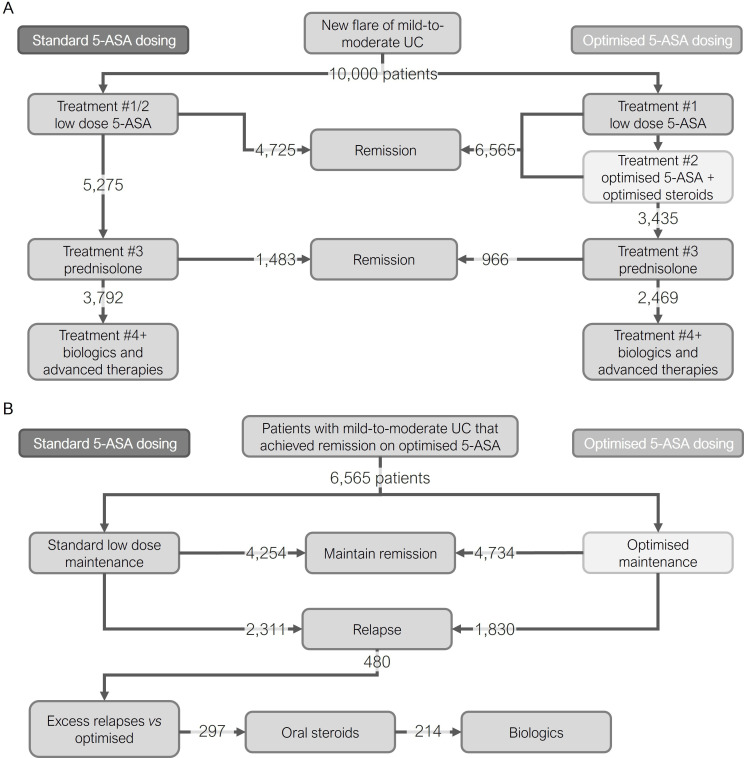
During induction, there was a 39% increase in patients achieving remission through the optimised pathway without requiring systemic steroids and/or biologics (6565 vs 4725 for standard). Potential steroidal/biological adverse events avoided included: seven venous thromboembolisms and eight serious infections. Out of the 6565 patients entering maintenance following successful induction on 5-ASA, there was a 21% reduction in relapses when optimised (1830 vs 2311 for standard). This translated into 297 patients avoiding further systemic steroids and 214 biologics. Optimisation led to an average net saving of £272 per patient entering the model for the induction and maintenance of remission over 1 year.
Modelling suggests that optimising 5-ASA therapy (both the inclusion of rectal 5-ASA into a combined oral and rectal regimen and maximisation of 5-ASA dose) has clinical and cost benefits that supports wider adoption in clinical practice.
5-氨基水杨酸(美沙拉嗪;5-ASA)是治疗轻度至中度溃疡性结肠炎(UC)的既定一线治疗药物。本研究旨在建立优化 5-ASA 治疗的模型。
通过诱导和 1 年的维持治疗,决策树模型对 10000 例新诊断为轻度至中度活动期 UC 的患者进行了随访。优化治疗(最大限度地提高 5-ASA 剂量并在治疗升级前使用口服和直肠联合治疗)与标准治疗(无优化的标准 5-ASA 剂量)进行了比较。模型数据来自已发表的荟萃分析。主要结局是达到并维持缓解的患者人数,同时作为次要结局对每种策略的治疗成本进行了分析(使用英国参考成本)。
在诱导期,通过优化途径,无需使用全身性皮质类固醇和/或生物制剂,达到缓解的患者增加了 39%(优化组为 6565 例,标准组为 4725 例)。避免了潜在的皮质类固醇/生物制剂不良事件包括:7 例静脉血栓栓塞和 8 例严重感染。在成功诱导 5-ASA 后进入维持治疗的 6565 例患者中,优化组的复发率降低了 21%(优化组为 1830 例,标准组为 2311 例)。这意味着有 297 例患者避免了进一步使用全身性皮质类固醇,214 例患者避免了使用生物制剂。优化治疗在诱导和维持缓解的 1 年中,平均每位进入模型的患者节省 272 英镑。
建模表明,优化 5-ASA 治疗(包括将直肠 5-ASA 纳入口服和直肠联合治疗方案以及最大化 5-ASA 剂量)具有临床和成本效益,支持在临床实践中更广泛地采用。