Thaker Rishi, Pink Kevin, Garapati Sita, Zarandi Donna, Shah Purvi, Ramasubbu Kumudha, Mehta Parag
Internal Medicine, New York-Presbyterian Brooklyn Methodist Hospital, Brooklyn, USA.
Cardiology, New York-Presbyterian Brooklyn Methodist Hospital, Brooklyn, USA.
Cureus. 2022 Jan 11;14(1):e21123. doi: 10.7759/cureus.21123. eCollection 2022 Jan.
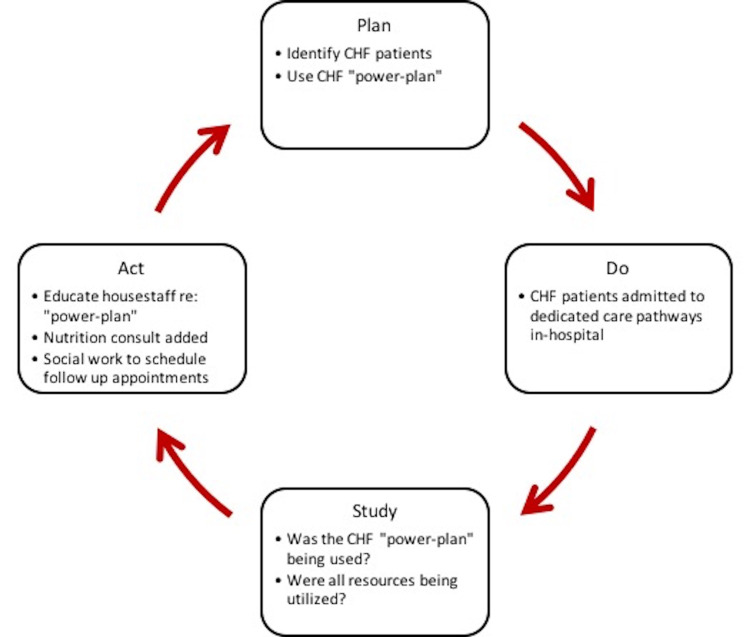
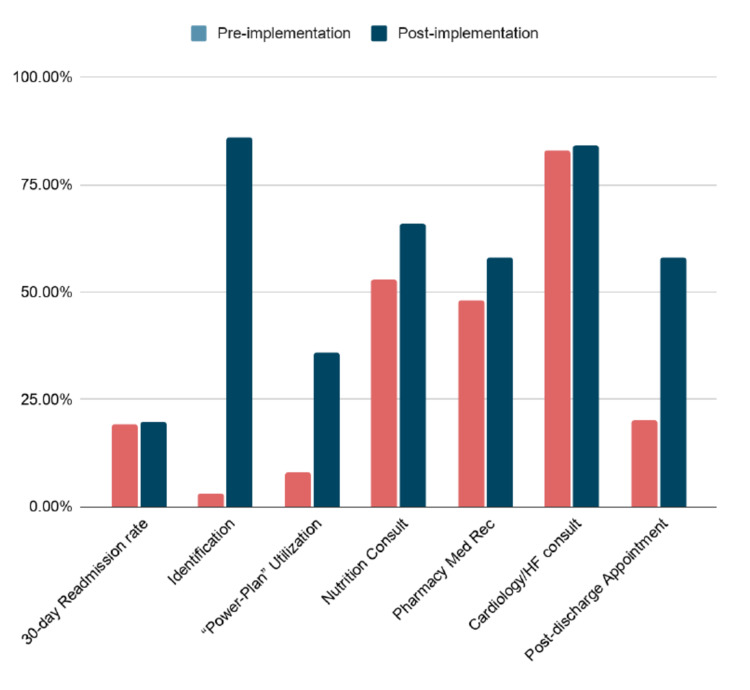
Introduction Heart failure accounts for 1-2% of overall healthcare costs. While the link between re-hospitalization and mortality is unclear, care pathways that standardize inpatient management and establish outpatient follow-up improve patient outcomes and reduce morbidity. Aim To implement a comprehensive interdisciplinary care pathway for heart failure patients with the goal of optimizing inpatient management and improving transitions of care. Methods To address this clinical need, New York-Presbyterian Brooklyn Methodist Hospital (NYP-BMH) identified resources needed to optimize patient care, developed an inpatient admission order set (so-called "power plan"), and implemented a multidisciplinary clinical care pathway. The Plan-Do-Study-Act cycle addressed the implementation obstacles. Interdisciplinary rounds guided day-to-day management and addressed barriers. Our team developed a sustainable care pathway, and measured the utilization of pharmacy, nutrition, physical therapy, case management, and social work resources; outpatient appointments were made prior to discharge. We used the Standards for Quality Improvement Reporting Excellence (SQUIRE) 2.0 guidelines to guide our planning and evaluation of this quality improvement initiative. Results Our intervention markedly increased the number of heart failure hospitalizations that were identified on admission, and the use of pharmacy/nutrition services was greater after the intervention. The utilization of our "power plan" promoted adherence to a series of evidence-based best practices, but these measures had no significant impact on readmissions as a whole. The involvement of the case management support team increased outpatient appointments made for patients prior to discharge and aided in the transition of care from inpatient to outpatient management. Conclusion The management of heart failure patients starts in the hospital and continues in the community. Patients who are treated in a standardized dedicated care pathway have reduced morbidity and better outcomes. Identifying these patients early, involving a comprehensive team, and transitioning their care to the outpatient setting improves the quality of care in these patients.
引言
心力衰竭占总体医疗费用的1%-2%。虽然再住院与死亡率之间的联系尚不清楚,但标准化住院管理并建立门诊随访的护理路径可改善患者预后并降低发病率。
目的
为心力衰竭患者实施全面的跨学科护理路径,以优化住院管理并改善护理过渡。
方法
为满足这一临床需求,纽约长老会布鲁克林卫理公会医院(NYP-BMH)确定了优化患者护理所需的资源,制定了住院入院医嘱集(即所谓的“强效计划”),并实施了多学科临床护理路径。计划-执行-研究-改进循环解决了实施障碍。跨学科查房指导日常管理并解决障碍。我们的团队制定了可持续的护理路径,并衡量了药学、营养、物理治疗、病例管理和社会工作资源的利用情况;出院前安排了门诊预约。我们使用卓越质量改进报告标准(SQUIRE)2.0指南来指导我们对这一质量改进举措的规划和评估。
结果
我们的干预显著增加了入院时确诊的心力衰竭住院病例数量,干预后药学/营养服务的使用增加。我们“强效计划”的实施促进了对一系列循证最佳实践的遵循,但这些措施对整体再入院率没有显著影响。病例管理支持团队的参与增加了为患者出院前安排的门诊预约,并有助于从住院护理向门诊管理的过渡。
结论
心力衰竭患者的管理始于医院并延续至社区。在标准化的专门护理路径中接受治疗的患者发病率降低,预后更好。早期识别这些患者,组建综合团队,并将其护理过渡到门诊环境可提高这些患者的护理质量。