GP Registrar, Primary Care Directorate, NHS Education for Scotland, Edinburgh, UK.
Ageing and Health, University of Dundee, Ninewells Hospital, Dundee, UK.
BMC Geriatr. 2018 Aug 28;18(1):197. doi: 10.1186/s12877-018-0883-3.
Recently hospitalized patients experience a period of generalized risk of adverse health events. This study examined reasons for, and predictors of, readmission to acute care facilities within 30 and 180 days of discharge from an inpatient rehabilitation unit for older people.
Routinely collected, linked clinical data on admissions to a single inpatient rehabilitation facility over a 13-year period were analysed. Data were available regarding demographics, comorbid disease, admission and discharge Barthel scores, length of hospital stay, and number of medications on discharge. Discharge diagnoses for the index admission and readmissions were available from hospital episode statistics. Univariate and multivariate Cox regression analyses were performed to identify baseline factors that predicted 30 and 180-day readmission.
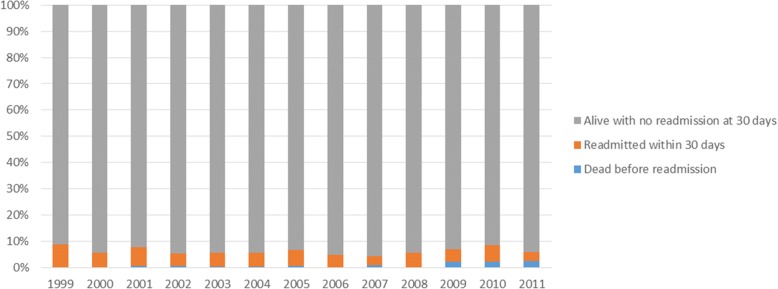
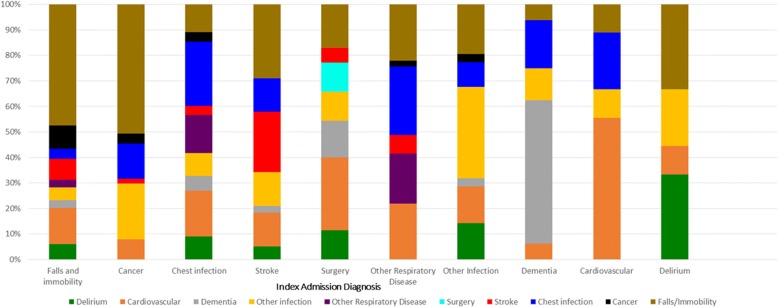
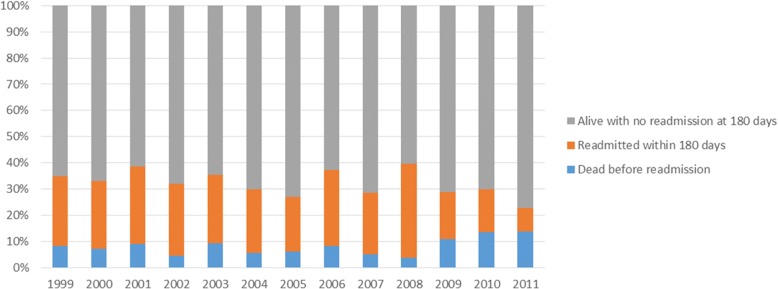
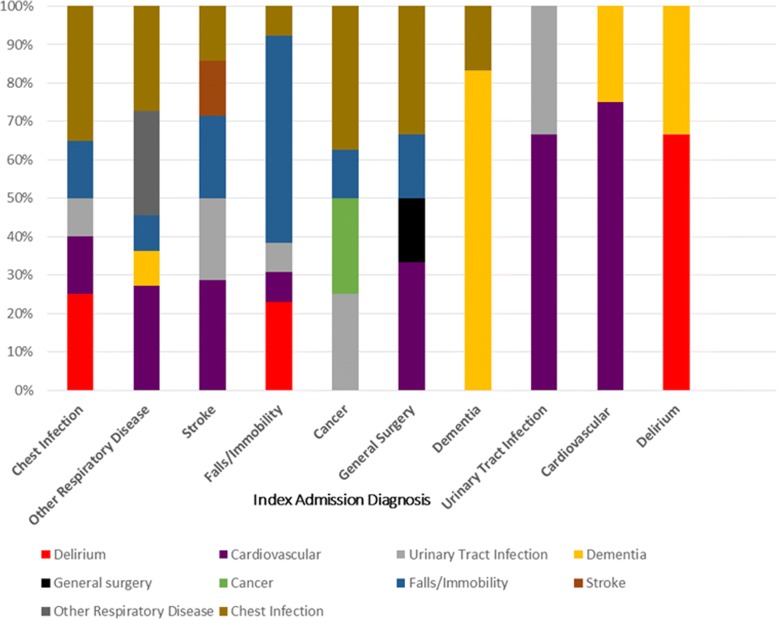
A total of 3984 patients were included in the analysis. The cohort had a mean age of 84.1 years (SD 7.4), and 39.7% were male. Overall, 5.6% (n = 222) and 23.2% (n = 926) of the patients were readmitted within 30 days and 180 days of discharge respectively. For patients readmitted to hospital, 26.6% and 21.1% of patients were readmitted with the same condition as their initial admission at 30 days and 180 respectively. For patients readmitted within 30 days, 13.5% (n = 30) were readmitted with the same condition with the most common diagnoses associated with readmission being chest infection, falls/immobility and stroke. For patients readmitted within 180 days, 12.4% (n = 115) of patients were readmitted with the same condition as the index condition with the most common diagnoses associated with readmission being falls/immobility, cancer and chest infections. In multivariable Cox regression analyses, older age, male sex, length of stay and heart failure predicted 30 or 180-day readmission. In addition, discharge from hospital to patients own home predicted 30-day readmission, whereas diagnoses of cancer, previous myocardial infarction or chronic obstructive pulmonary disease predicted 180-day readmission.
Most readmissions of older people after discharge from inpatient rehabilitation occurred for different reasons to the original hospital admission. Patterns of predictors for early and late readmission differed, suggesting the need for different mitigation strategies.
最近住院的患者经历了一段全身性不良健康事件的风险期。本研究旨在探讨老年人住院康复单元出院后 30 天和 180 天内再次入住急性护理设施的原因和预测因素。
对一家住院康复机构 13 年来的常规收集、链接的临床入院数据进行了分析。数据包括人口统计学、合并症、入院和出院 Barthel 评分、住院时间和出院时的药物数量。索引入院和再入院的出院诊断可从医院入院统计数据中获得。进行单变量和多变量 Cox 回归分析,以确定预测 30 天和 180 天再入院的基线因素。
共纳入 3984 名患者进行分析。该队列的平均年龄为 84.1 岁(标准差 7.4),39.7%为男性。总体而言,5.6%(n=222)和 23.2%(n=926)的患者在出院后 30 天和 180 天内再次入院。对于再次入院的患者,26.6%和 21.1%的患者在 30 天和 180 天的再次入院时的情况与首次入院时相同。对于 30 天内再次入院的患者,13.5%(n=30)的患者因与初次入院相同的情况再次入院,最常见的与再次入院相关的诊断为肺炎、跌倒/失能和中风。对于 180 天内再次入院的患者,12.4%(n=115)的患者因与索引条件相同的情况再次入院,最常见的与再次入院相关的诊断为跌倒/失能、癌症和肺炎。在多变量 Cox 回归分析中,年龄较大、男性、住院时间和心力衰竭预测 30 天或 180 天的再入院。此外,出院回家预测 30 天的再入院,而癌症、先前的心肌梗死或慢性阻塞性肺疾病的诊断预测 180 天的再入院。
老年人从住院康复出院后,大多数再次入院的原因与初次入院不同。早期和晚期再入院的预测因素模式不同,这表明需要采取不同的缓解策略。