Lee Todd C, Morris Andrew M, Grover Steven A, Murthy Srinivas, McDonald Emily G
Division of Infectious Diseases, Department of Medicine, McGill University Health Centre, Montréal, Québec, Canada.
Clinical Practice Assessment Unit, Department of Medicine, McGill University Health Centre, Montréal, Québec, Canada.
Open Forum Infect Dis. 2022 Jan 19;9(3):ofac008. doi: 10.1093/ofid/ofac008. eCollection 2022 Mar.
Several outpatient coronavirus disease 2019 (COVID-19) therapies have reduced hospitalization in randomized controlled trials. The choice of therapy may depend on drug efficacy, toxicity, pricing, availability, and available infrastructure. To facilitate comparative decision-making, we evaluated the efficacy of each treatment in clinical trials and estimated the cost per hospitalization prevented.
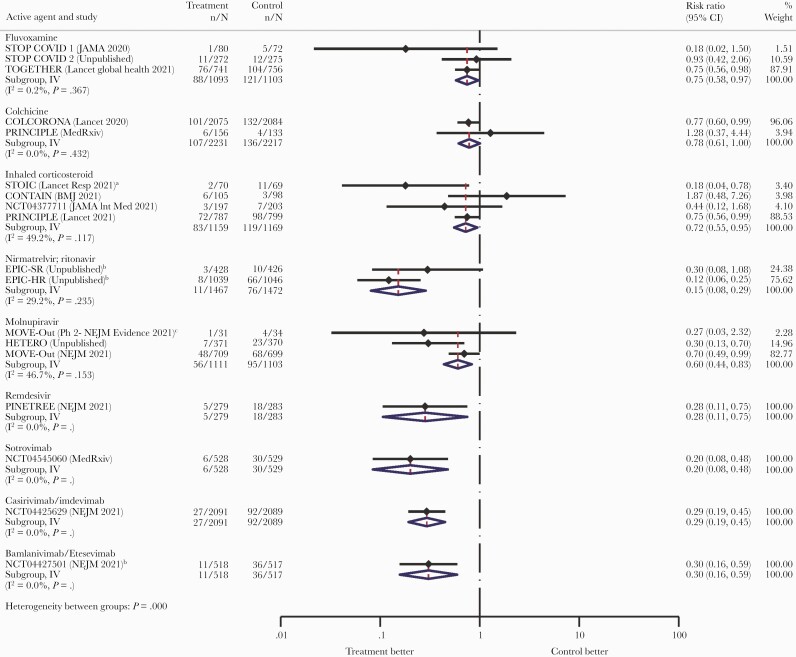
Wherever possible, we obtained relative risk for hospitalization from published randomized controlled trials. Otherwise, we extracted data from press releases, conference abstracts, government submissions, or preprints. If there was >1 study, the results were meta-analyzed. Using relative risk, we estimated the number needed to treat (NNT), assuming a baseline hospitalization risk of 5%, and compared the cost per hospitalization prevented with the estimate for an average Medicare COVID-19 hospitalization ($21 752). Drug pricing was estimated from GoodRx, from government purchases, or manufacturer estimates. Administrative and societal costs were not included. Results will be updated online as new studies emerge and/or final numbers become available.
At a 5% risk of hospitalization, the estimated NNT was 80 for fluvoxamine, 91 for colchicine, 72 for inhaled corticosteroids, 24 for nirmatrelvir/ritonavir, 50 for molnupiravir, 28 for remdesivir, 25 for sotrovimab, 29 for casirivimab/imdevimab, and 29 for bamlanivimab/etesevimab. For drug cost per hospitalization prevented, colchicine, fluvoxamine, inhaled corticosteroids, and nirmatrelvir/ritonavir were below the Medicare estimated hospitalization cost.
Many countries are fortunate to have access to several effective outpatient therapies to prevent COVID-19 hospitalization. Given differences in efficacy, toxicity, cost, and administration complexity, this assessment serves as one means to frame treatment selection.
在随机对照试验中,几种新型冠状病毒肺炎(COVID-19)门诊治疗方法可减少住院率。治疗方法的选择可能取决于药物疗效、毒性、价格、可及性和可用基础设施。为便于进行比较决策,我们评估了每种治疗方法在临床试验中的疗效,并估算了预防每次住院的成本。
只要有可能,我们就从已发表的随机对照试验中获取住院的相对风险。否则,我们从新闻稿、会议摘要、政府提交的资料或预印本中提取数据。如果有超过1项研究,则对结果进行荟萃分析。利用相对风险,我们估算了治疗所需人数(NNT),假设基线住院风险为5%,并将预防每次住院的成本与医疗保险COVID-19住院平均费用估计值(21752美元)进行比较。药物价格根据GoodRx、政府采购或制造商估计值估算。未包括行政和社会成本。随着新研究的出现和/或最终数据的可得,结果将在网上更新。
在5%的住院风险下,氟伏沙明的估计NNT为80,秋水仙碱为91,吸入性糖皮质激素为72,奈玛特韦/利托那韦为24,莫努匹拉韦为50,瑞德西韦为28,索托维单抗为25,卡西瑞韦/伊德维单抗为29,巴姆兰尼单抗/依替塞韦单抗为29。对于预防每次住院的药物成本,秋水仙碱、氟伏沙明、吸入性糖皮质激素和奈玛特韦/利托那韦低于医疗保险估计的住院成本。
许多国家有幸能够获得几种有效的门诊治疗方法来预防COVID-19住院。鉴于疗效、毒性、成本和给药复杂性存在差异,本评估可作为指导治疗选择的一种方法。