Department of Health Sciences, Faculty of Science, Vrije Universiteit Amsterdam, De Boelelaan 1085, 1081 HV, Amsterdam, The Netherlands.
Zilveren Kruis (Achmea), Handelsweg 2, 3707 NH, Zeist, The Netherlands.
BMC Health Serv Res. 2022 Feb 15;22(1):208. doi: 10.1186/s12913-022-07527-z.
Patients having forgone healthcare because of the costs involved has become more prevalent in recent years. Certain patient characteristics, such as income, are known to be associated with a stronger demand-response to cost-sharing. In this study, we first assess the relative importance of patient characteristics with regard to having forgone healthcare due to cost-sharing payments, and then employ qualitative methods in order to understand these findings better.
Survey data was collected from a Dutch panel of regular users of healthcare. Logistic regression models and dominance analyses were performed to assess the relative importance of patient characteristics, i.e., personal characteristics, health, educational level, sense of mastery and financial situation. Semi-structured interviews (n = 5) were conducted with those who had forgone healthcare. The verbatim transcribed interviews were thematically analyzed.
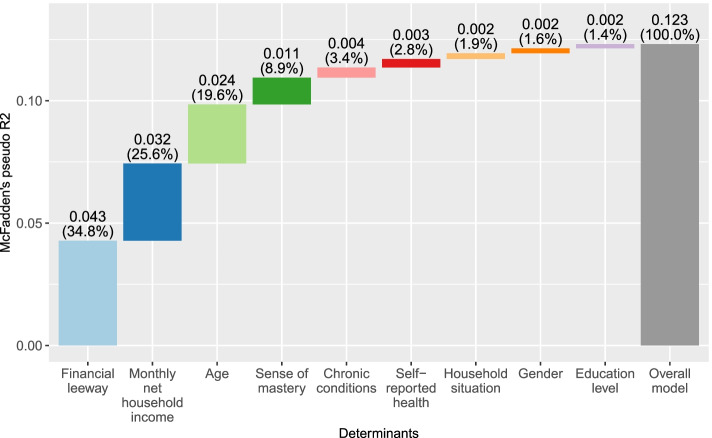
Of the 7,339 respondents who completed the questionnaire, 1,048 respondents (14.3%) had forgone healthcare because of the deductible requirement. The regression model indicated that having a higher income reduced the odds of having forgone recommended healthcare due to the deductible (odds ratios of higher income categories relative to the lowest income category (reference): 0.29-0.49). However, dominance analyses revealed that financial leeway was more important than income: financial leeway contributed the most (34.8%) to the model's overall McFadden's pseudo-R2 (i.e., 0.123), followed by income (25.6%). Similar results were observed in stratified models and in population weighted models. Qualitative analyses distinguished four main themes that affected the patient's decision whether to use healthcare: financial barriers, structural barriers related to the complex design of cost-sharing programs, individual considerations of the patient, and the perceived lack of control regarding treatment choices within a given treatment trajectory. Furthermore, "having forgone healthcare" seemed to have a negative connotation.
Our findings show that financial leeway is more important than income with respect to having forgone recommended healthcare due to cost-sharing payments, and that other factors such as the perceived necessity of healthcare also matter. Our findings imply that solely adapting cost-sharing programs to income levels will only get one so far. Our study underlines the need for a broader perspective in the design of cost-sharing programs.
近年来,由于费用问题而放弃医疗保健的患者越来越多。某些患者特征,如收入,与对成本共付的更强需求反应有关。在这项研究中,我们首先评估了患者特征对于因成本共付而放弃医疗保健的相对重要性,然后采用定性方法来更好地理解这些发现。
从荷兰医疗保健的常规使用者小组中收集了调查数据。使用逻辑回归模型和优势分析来评估患者特征的相对重要性,即个人特征、健康、教育水平、掌控感和财务状况。对因扣除额要求而放弃医疗保健的人进行了(n=5)半结构访谈。对逐字记录的访谈进行了主题分析。
在完成问卷的 7339 名受访者中,有 1048 名受访者(14.3%)因扣除额要求而放弃了医疗保健。回归模型表明,较高的收入降低了因扣除额而放弃推荐的医疗保健的可能性(相对于最低收入类别,较高收入类别的优势比(OR):0.29-0.49)。然而,优势分析表明,财务余地比收入更为重要:财务余地对模型整体麦克法登伪 R2 的贡献最大(34.8%)(即 0.123),其次是收入(25.6%)。在分层模型和人口加权模型中观察到了类似的结果。定性分析区分了影响患者是否使用医疗保健的四个主要主题:经济障碍、与成本共付计划复杂设计相关的结构性障碍、患者的个人考虑因素、以及在特定治疗轨迹内对治疗选择缺乏控制的看法。此外,“放弃医疗保健”似乎带有负面含义。
我们的研究结果表明,与因成本共付而放弃推荐的医疗保健相比,财务余地比收入更为重要,而其他因素,如对医疗保健的必要性的看法也很重要。我们的研究结果表明,仅根据收入水平调整成本共付计划是远远不够的。我们的研究强调了在设计成本共付计划时需要更广泛的视角。