Department of Orthopedic Surgery, North Medical Center, Kyoto Prefectural University of Medicine, Kyoto, Japan.
Department of Orthopedics, Graduate School of Medical Science, Kyoto Prefectural University of Medicine, Kyoto, Japan.
J Cachexia Sarcopenia Muscle. 2022 Apr;13(2):945-954. doi: 10.1002/jcsm.12940. Epub 2022 Feb 15.
The sarcopenia index (SI), calculated as the ratio of serum creatinine to cystatin C levels, reflects skeletal muscle mass and strength. Patients with hip fracture (HF) and sarcopenia have poor functional outcomes, and many require long-term care after surgery. We hypothesized that the SI can predict preoperative and early postoperative functional outcomes.
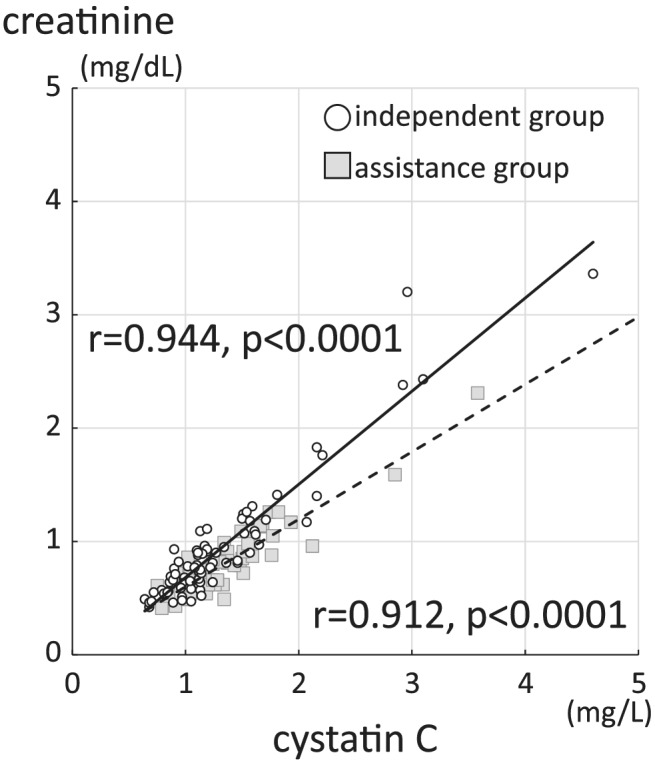
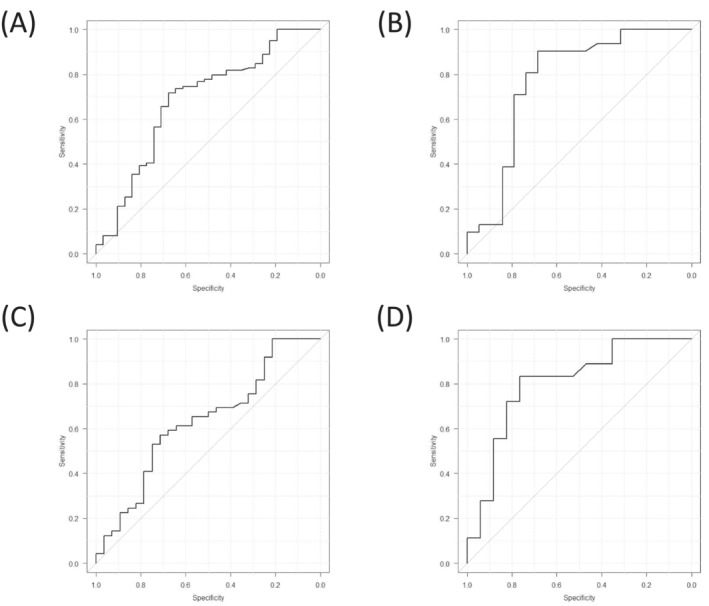
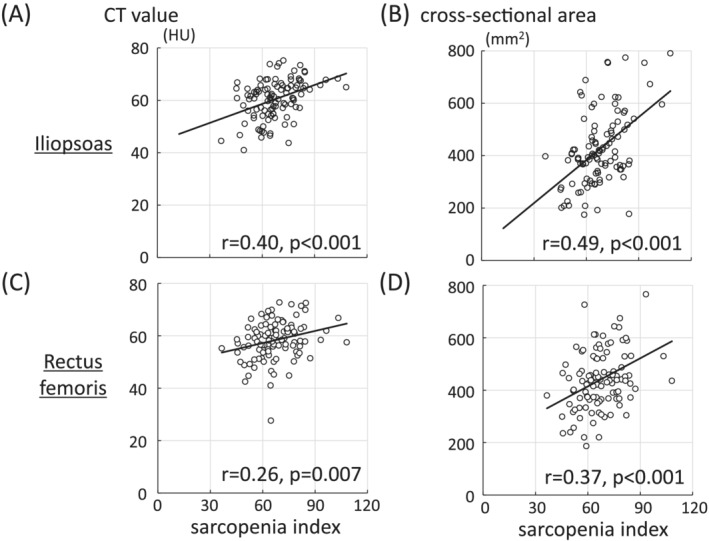
Preoperative serum creatinine and cystatin C were measured to calculate the SI for patients with surgically treated HF (n = 130, mean age: 87.8 ± 6.9 years). Walking ability before and 2 weeks after surgery was assessed, and patients were dichotomized into independent and assistance groups. To assess the validity of the SI, we examined its correlation with the quality [computed tomography (CT) value] and quantity (cross-sectional area) of the muscles around the hip on the non-operated side, which were preoperatively measured using CT. Receiver operating characteristic (ROC) analysis was performed to evaluate the prognostic value of the SI.
The SI of the preoperative independent (n = 77) and assistance groups (n = 53) significantly differed (70.2 ± 12.4 and 60.1 ± 9.8, respectively, P < 0.000001). At 2 weeks after surgery, the SI was significantly higher in the independent group (n = 31, 73.0 ± 14.9) than in the assistance group (n = 99, 64.0 ± 10.7, P = 0.0003). In the preoperative independent group, 28 could walk independently after surgery (SI: 74.8 ± 14.0) while 49 required assistance (SI: 67.7 ± 10.6, P = 0.01). For patients with femoral neck fracture (FNF), the SIs were significantly higher in the postoperative independent group (78.6 ± 15.7) than in the postoperative assistance group (63.2 ± 10.9, P = 0.002). Logistic regression analysis showed that the odds ratio (95% confidence interval) of the SI for postoperative walking ability was 0.95 (0.91-0.99, P = 0.03). The correlations of SIs with CT values and cross-sectional areas were as follows: iliopsoas at the apex of the femoral head, r = 0.40, P < 0.001 and r = 0.49, P < 0.001, respectively; rectus femoris at the level of the lessor trochanter, r = 0.26, P = 0.007 and r = 0.37, P < 0.001, respectively. ROC analysis for predicting postoperative walking ability in preoperative independent patients with HF and FNF revealed areas under the curve (95% confidence interval) of 0.63 (0.50-0.76) and 0.80 (0.65-0.96), respectively.
In patients with HF, the SI correlated with preoperative walking ability and could predict postoperative walking ability. Among patients who could walk independently before surgery, those with high SIs could walk independently early in the postoperative period. The SI is beneficial for estimating walking ability in patients with HF.
肌少症指数(SI)通过血清肌酐与胱抑素 C 的比值计算得出,反映了骨骼肌的质量和力量。患有髋部骨折(HF)和肌少症的患者功能预后较差,许多患者在手术后需要长期护理。我们假设 SI 可以预测术前和术后早期的功能结果。
测量了接受手术治疗的 HF 患者(n=130,平均年龄:87.8±6.9 岁)的术前血清肌酐和胱抑素 C,以计算 SI。评估了术前和术后 2 周的步行能力,并将患者分为独立和辅助两组。为了评估 SI 的有效性,我们检查了其与髋关节未手术侧肌肉质量(使用 CT 值评估)和数量(横截面积)的相关性,这些数据在术前使用 CT 进行了测量。进行了接受者操作特征(ROC)分析,以评估 SI 的预后价值。
术前独立(n=77)和辅助组(n=53)的 SI 显著不同(分别为 70.2±12.4 和 60.1±9.8,P<0.000001)。术后 2 周,独立组(n=31,73.0±14.9)的 SI 明显高于辅助组(n=99,64.0±10.7,P=0.0003)。在术前独立组中,28 人在手术后可以独立行走(SI:74.8±14.0),而 49 人需要辅助(SI:67.7±10.6,P=0.01)。对于股骨颈骨折(FNF)患者,术后独立组的 SI(78.6±15.7)明显高于术后辅助组(63.2±10.9,P=0.002)。逻辑回归分析显示,SI 对术后行走能力的比值比(95%置信区间)为 0.95(0.91-0.99,P=0.03)。SI 与 CT 值和横截面积的相关性如下:股骨头顶点的髂腰肌,r=0.40,P<0.001 和 r=0.49,P<0.001;小转子水平的股直肌,r=0.26,P=0.007 和 r=0.37,P<0.001。HF 和 FNF 术前独立患者术后行走能力的 ROC 分析显示,曲线下面积(95%置信区间)分别为 0.63(0.50-0.76)和 0.80(0.65-0.96)。
在 HF 患者中,SI 与术前步行能力相关,可预测术后步行能力。在术前可独立行走的患者中,SI 较高的患者在术后早期可独立行走。SI 有助于评估 HF 患者的步行能力。